

Central sleep apnea: Pathophysiology and treatment
- PMID: 17296668
- PMCID: PMC2287191
- DOI: 10.1378/chest.06.2287
Central sleep apnea: Pathophysiology and treatment
Abstract
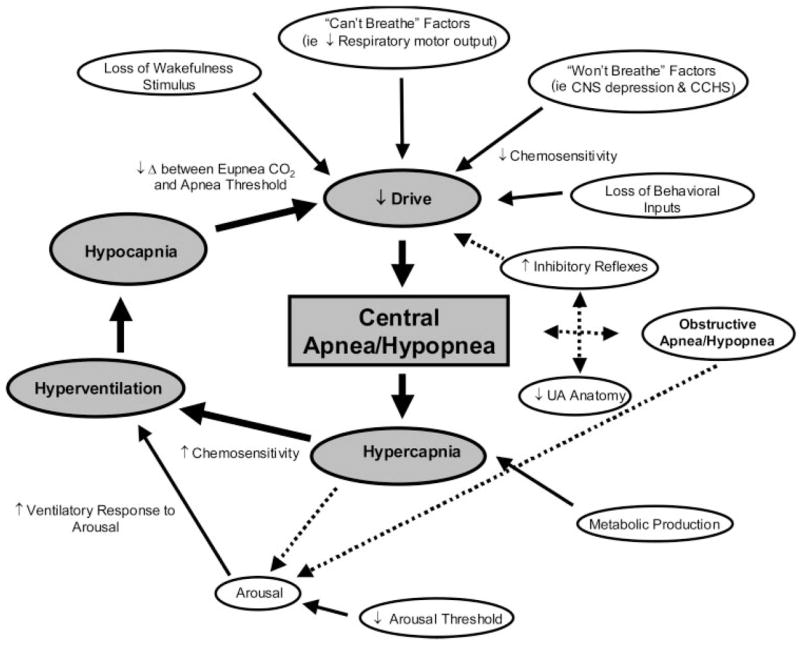
Central sleep apnea (CSA) is characterized by a lack of drive to breathe during sleep, resulting in repetitive periods of insufficient ventilation and compromised gas exchange. These nighttime breathing disturbances can lead to important comorbidity and increased risk of adverse cardiovascular outcomes. There are several manifestations of CSA, including high altitude-induced periodic breathing, idiopathic CSA, narcotic-induced central apnea, obesity hypoventilation syndrome, and Cheyne-Stokes breathing. While unstable ventilatory control during sleep is the hallmark of CSA, the pathophysiology and the prevalence of the various forms of CSA vary greatly. This brief review summarizes the underlying physiology and modulating components influencing ventilatory control in CSA, describes the etiology of each of the various forms of CSA, and examines the key factors that may exacerbate apnea severity. The clinical implications of improved CSA pathophysiology knowledge and the potential for novel therapeutic treatment approaches are also discussed.
Figures
References
-
- Lanfranchi PA, Somers VK, Braghiroli A, et al. Central sleep apnea in left ventricular dysfunction: prevalence and implications for arrhythmic risk. Circulation. 2003;107:727–732. - PubMed
-
- Javaheri S, Parker TJ, Liming JD, et al. Sleep apnea in 81 ambulatory male patients with stable heart failure: types and their prevalences, consequences, and presentations. Circulation. 1998;97:2154–2159. - PubMed
-
- White DP, Gleeson K, Pickett CK, et al. Altitude acclimatization: influence on periodic breathing and chemoresponsiveness during sleep. J Appl Physiol. 1987;63:401–412. - PubMed
-
- Malhotra A, Berry RB, White DP. Central sleep apnea. In: Carney PR, Berry RB, Geyer JD, editors. Clinical sleep disorders. Philadelphia, PA: Lippincott Williams and Wilkins; 2004. pp. 331–346.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
