

Maternal mortality and severe morbidity associated with low-risk planned cesarean delivery versus planned vaginal delivery at term
- PMID: 17296957
- PMCID: PMC1800583
- DOI: 10.1503/cmaj.060870
Maternal mortality and severe morbidity associated with low-risk planned cesarean delivery versus planned vaginal delivery at term
Abstract
Background: The rate of elective primary cesarean delivery continues to rise, owing in part to the widespread perception that the procedure is of little or no risk to healthy women.
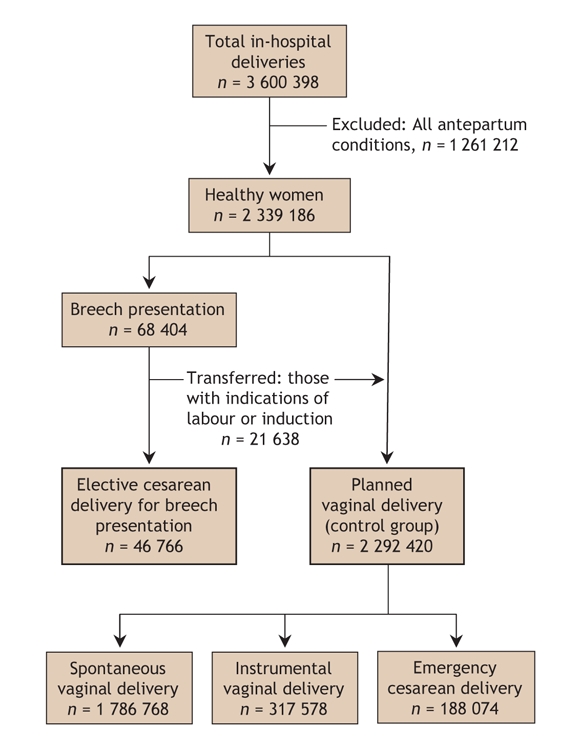
Methods: Using the Canadian Institute for Health Information's Discharge Abstract Database, we carried out a retrospective population-based cohort study of all women in Canada (excluding Quebec and Manitoba) who delivered from April 1991 through March 2005. Healthy women who underwent a primary cesarean delivery for breech presentation constituted a surrogate "planned cesarean group" considered to have undergone low-risk elective cesarean delivery, for comparison with an otherwise similar group of women who had planned to deliver vaginally.
Results: The planned cesarean group comprised 46,766 women v. 2,292,420 in the planned vaginal delivery group; overall rates of severe morbidity for the entire 14-year period were 27.3 and 9.0, respectively, per 1000 deliveries. The planned cesarean group had increased postpartum risks of cardiac arrest (adjusted odds ratio [OR] 5.1, 95% confidence interval [CI] 4.1-6.3), wound hematoma (OR 5.1, 95% CI 4.6-5.5), hysterectomy (OR 3.2, 95% CI 2.2-4.8), major puerperal infection (OR 3.0, 95% CI 2.7-3.4), anesthetic complications (OR 2.3, 95% CI 2.0-2.6), venous thromboembolism (OR 2.2, 95% CI 1.5-3.2) and hemorrhage requiring hysterectomy (OR 2.1, 95% CI 1.2-3.8), and stayed in hospital longer (adjusted mean difference 1.47 d, 95% CI 1.46-1.49 d) than those in the planned vaginal delivery group, but a lower risk of hemorrhage requiring blood transfusion (OR 0.4, 95% CI 0.2-0.8). Absolute risk increases in severe maternal morbidity rates were low (e.g., for postpartum cardiac arrest, the increase with planned cesarean delivery was 1.6 per 1000 deliveries, 95% CI 1.2-2.1). The difference in the rate of in-hospital maternal death between the 2 groups was nonsignificant (p = 0.87).
Interpretation: Although the absolute difference is small, the risks of severe maternal morbidity associated with planned cesarean delivery are higher than those associated with planned vaginal delivery. These risks should be considered by women contemplating an elective cesarean delivery and by their physicians.
Figures
Comment in
-
Is planned cesarean childbirth a safe alternative?CMAJ. 2007 Feb 13;176(4):475-6. doi: 10.1503/cmaj.061724. CMAJ. 2007. PMID: 17296960 Free PMC article. No abstract available.
-
Analyzing the risks of cesarean delivery.CMAJ. 2007 Oct 9;177(8):899. doi: 10.1503/cmaj.1070051. CMAJ. 2007. PMID: 17923661 Free PMC article. No abstract available.
References
-
- National Institutes of Health state-of-the science conference statement: cesarean delivery on maternal request March 27–29, 2006. Obstet Gynecol 2006;107:1386-97. - PubMed
-
- Canadian Institute for Health Information. Health indicators, 2005. Available: http://dsp-psd.pwgsc.gc.ca/Collection/H115-16-2005E.pdf (accessed 2006 Nov 20).
-
- Health Canada. Canadian perinatal health report 2003. Ottawa: Minister of Public Works and Government Services Canada; 2003. Available: www.phac-aspc.gc.ca/publicat/cphr-rspc03/pdf/cphr-rspc03_e.pdf (accessed 2006 Nov 20).
-
- Women's Health Care Physicians, Task Force on Cesarean Delivery Rates. Evaluation of cesarean delivery. Washington: American College of Obstetricians and Gynecologists; 2000.
-
- Scott JR. Cesarean delivery on request: Where do we go from here? Obstet Gynecol 2006;107:1222-3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous