

Intracranial vascular anomalies in patients with periorbital lymphatic and lymphaticovenous malformations
- PMID: 17297008
- PMCID: PMC7977401
Intracranial vascular anomalies in patients with periorbital lymphatic and lymphaticovenous malformations
Abstract
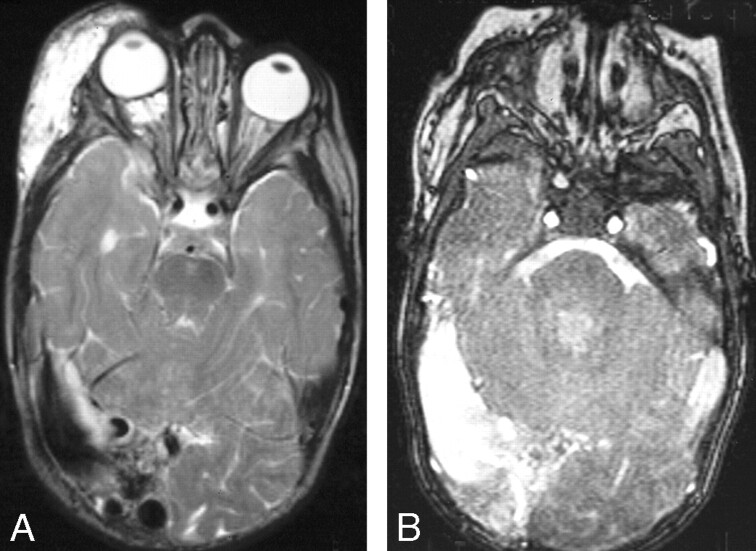
Background and purpose: The purpose of this study was to determine the nature, incidence, and radiologic appearance of intracranial vascular anomalies that occur in association with periorbital lymphatic malformation (LM) and lymphaticovenous malformation (LVM).
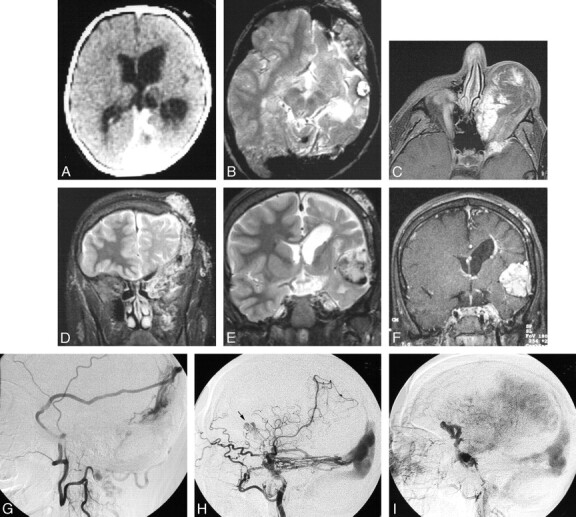
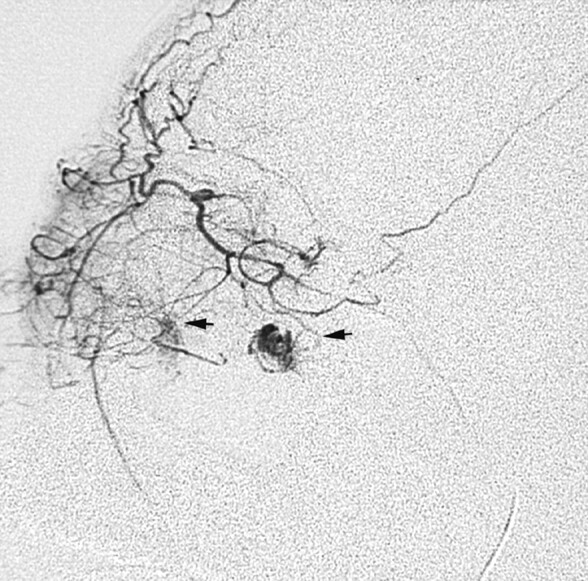
Materials and methods: We retrospectively reviewed clinical records and imaging studies of 33 patients ranging in age from the neonatal period to 39 years (mean age, 5.1 years; median age, 1.0 year) who were evaluated for orbital LM or LVM at our institution between 1953 and 2002. Imaging studies, including CT, MR imaging, and cerebral angiograms, were evaluated by 2 radiologists to determine morphologic features of orbital LM and to identify associated noncontiguous intracranial vascular and parenchymal anomalies, including arteriovenous malformations (AVM), cerebral cavernous malformations (CCM), developmental venous anomalies (DVA), dural arteriovenous malformations (DAVM), and sinus pericranii (SP).
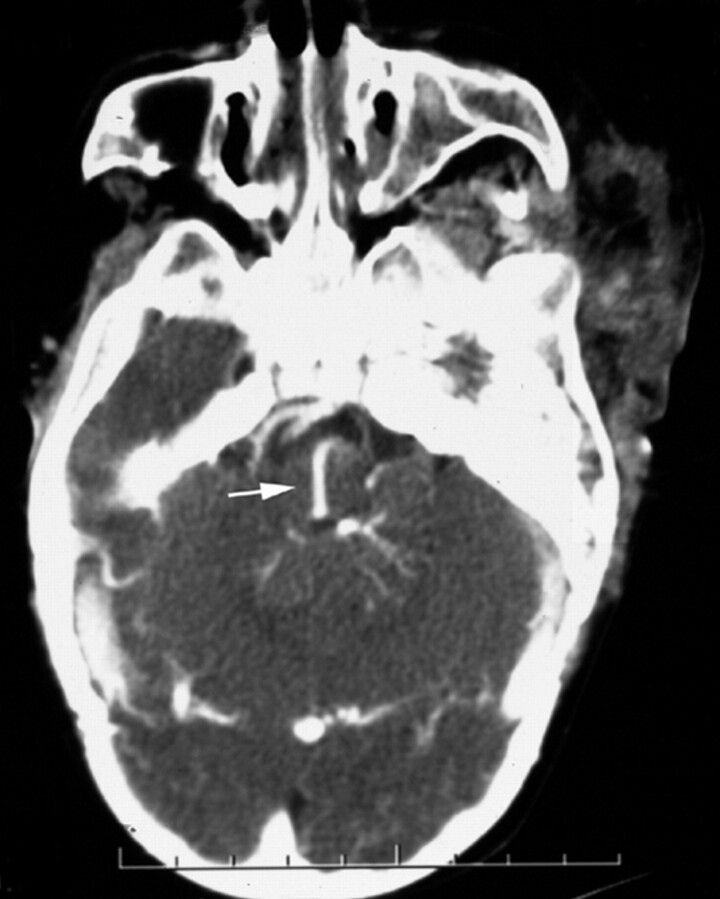
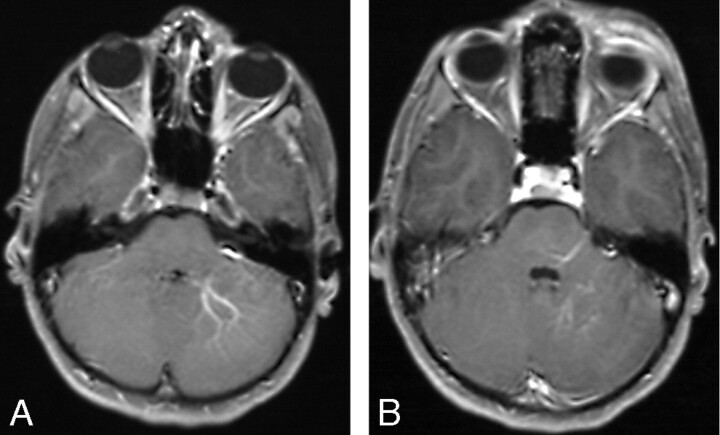
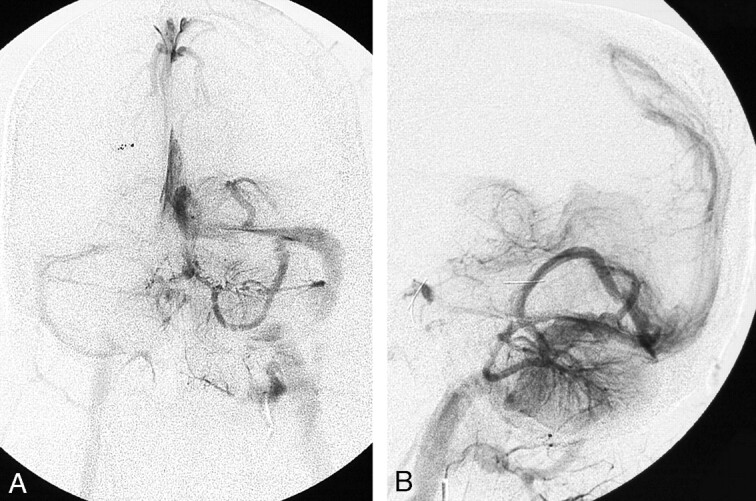
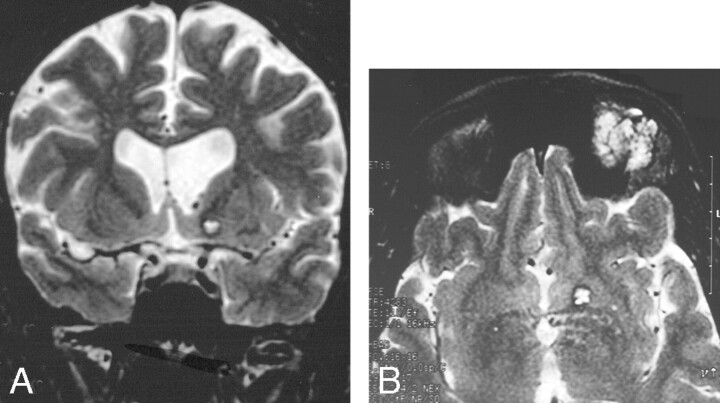
Results: The malformation was left-sided in 70% of patients. Twenty-two patients (70%) had intracranial vascular anomalies: DVA (n = 20; 61%), CCM (n = 2; 6%), DAVM (n = 4; 12%), pial AVM (n = 1; 3%), and SP (n = 1; 3%). Arterial shunts were present in the soft tissues in 2 patients (6%). Three patients had jugular venous anomalies. Three patients (9%) had cerebral hemiatrophy, 2 (6%) had focal cerebral atrophy, and 2 had Chiari I malformation.
Conclusions: Intracranial vascular anomalies, some of which are potentially symptomatic and require treatment, are present in more than two thirds of patients with periorbital LM. Initial imaging of patients with orbital LM should include the brain as well as the orbit.
Figures
References
-
- Katz SE, Rootman J, Vangveeravong S, et al. Combined venous lymphatic malformations of the orbit (so-called lymphangiomas). Association with noncontiguous intracranial vascular anomalies. Ophthalmology 1998;105:176–84 - PubMed
-
- Greene AK, Burrows PE, Smith L, et al. Periorbital lymphatic malformation: clinical course and management in 42 patients. Plast Reconstr Surg 2005;115:22–30 - PubMed
-
- Coll GE, Goldberg RA, Krauss H, et al. Concomitant lymphangioma and arteriovenous malformation of the orbit. Am J Ophthalmol 1991;112:200–05 - PubMed
-
- Graeb DA, Rootman J, Robertson WD, et al. Orbital lymphangiomas: clinical, radiologic, and pathologic characteristics. Radiology 1990;175:417–21 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical