

Survival analysis of Korean end-stage renal disease patients according to renal replacement therapy in a single center
- PMID: 17297256
- PMCID: PMC2693574
- DOI: 10.3346/jkms.2007.22.1.81
Survival analysis of Korean end-stage renal disease patients according to renal replacement therapy in a single center
Abstract
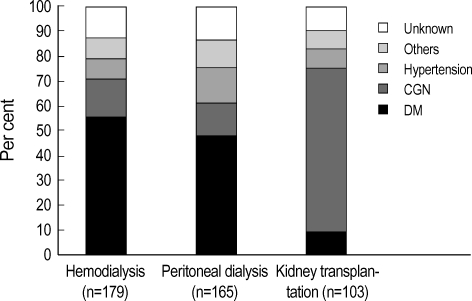
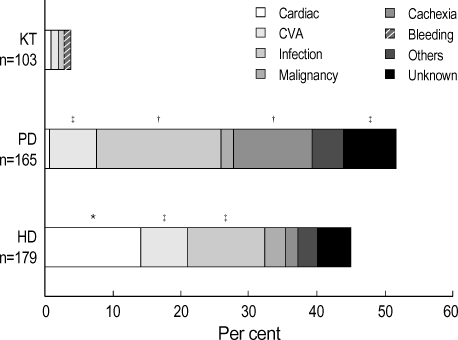
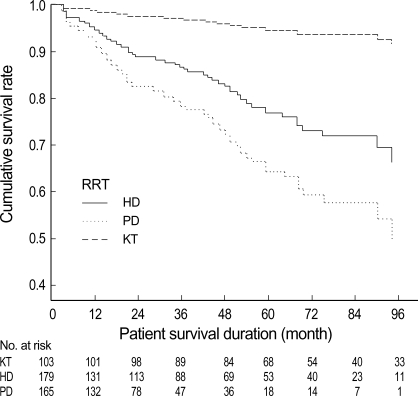
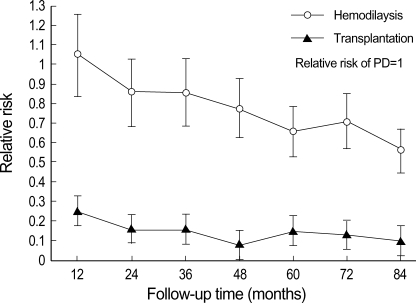
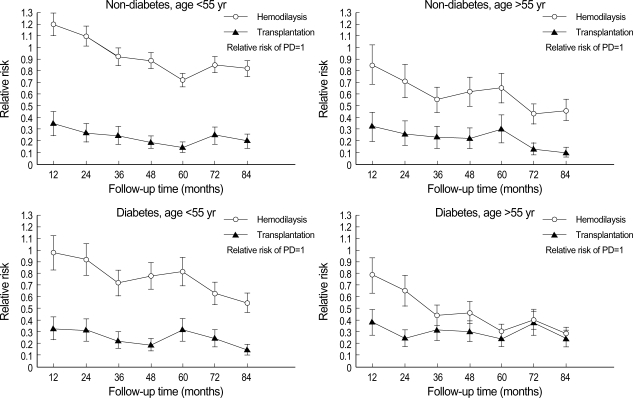
This study was to investigate clinical characteristics and any differential trends in survival among renal replacement therapy (hemodialysis [HD], peritoneal dialysis [PD], and kidney transplantation [KT]) in Korean end-stage renal disease (ESRD) population. We tried to analyze retrospectively the survival rate adjusted by risk factors and the relative risk stratified by key risk factors among 447 ESRD patients who began dialysis or had a kidney transplant at Ajou University Hospital from 1994 to 2004. In adjusted Cox survival curves, the KT patients had the best survival rate, and the HD patients had better survival than PD patients. The consistent trends in different subgroups stratified by age and diabetes were as following: 1) The risk of death for PD and HD was not proportional over time, 2) The relative risk of PD was similar or lower than that of HD for the first 12 months, but it became higher at later period. The significant predictors for mortality were age (over 55 yr), presence of diabetes, cerebrovascular accident at ESRD onset, and more than one time of hospitalization caused by malnutrition. Further large-scaled, multicenter-based comparative study is needed in Korean ESRD patients and more meticulous attention is required in high-risk patients.
Figures
Similar articles
-
Comparative study of renal replacement therapy in Korean diabetic end-stage renal disease patients: a single center study.Yonsei Med J. 2003 Jun 30;44(3):454-62. doi: 10.3349/ymj.2003.44.3.454. Yonsei Med J. 2003. PMID: 12833583
-
Hemodialysis and peritoneal dialysis are associated with similar outcomes for end-stage renal disease treatment in Canada.Nephrol Dial Transplant. 2012 Sep;27(9):3568-75. doi: 10.1093/ndt/gfr674. Epub 2012 Mar 5. Nephrol Dial Transplant. 2012. PMID: 22391139
-
[REIN Report 2011--summary].Nephrol Ther. 2013 Sep;9 Suppl 1:S3-6. doi: 10.1016/S1769-7255(13)70036-1. Nephrol Ther. 2013. PMID: 24119584 French.
-
Optimizing end-stage renal disease therapy for the patient with diabetes mellitus.Semin Nephrol. 1997 Jul;17(4):331-45. Semin Nephrol. 1997. PMID: 9241718 Review.
-
Renal replacement therapy in Korea, 2012.Kidney Res Clin Pract. 2014 Mar;33(1):9-18. doi: 10.1016/j.krcp.2014.01.002. Epub 2014 Mar 12. Kidney Res Clin Pract. 2014. PMID: 26877945 Free PMC article. Review.
Cited by
-
Impact of dialysis modality on technique survival in end-stage renal disease patients.Korean J Intern Med. 2016 Jan;31(1):106-15. doi: 10.3904/kjim.2016.31.1.106. Epub 2015 Dec 28. Korean J Intern Med. 2016. PMID: 26767864 Free PMC article.
-
Propensity-matched mortality comparison of incident hemodialysis and peritoneal dialysis patients.J Am Soc Nephrol. 2010 Mar;21(3):499-506. doi: 10.1681/ASN.2009060635. Epub 2010 Feb 4. J Am Soc Nephrol. 2010. PMID: 20133483 Free PMC article.
-
Comparison of patients starting hemodialysis with those underwent hemodialysis 15 years ago at the same dialysis center in Korea.Korean J Intern Med. 2010 Jun;25(2):188-94. doi: 10.3904/kjim.2010.25.2.188. Epub 2010 Jun 1. Korean J Intern Med. 2010. PMID: 20526393 Free PMC article.
References
-
- US Renal Data System. USRDS 2004 Annual Data Report: Atlas of End Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Disease. 2005. Mar,
-
- Canadian Organ Replacement Register. 1993 Annual Report. Don Mills, ON: Canadian Institute for Health Information; 1995. Mar,
-
- Bloembergen WE, Port FK, Mauger EA, Wolfe RA. A comparison of mortality between patients treated with hemodialysis and peritoneal dialysis. J Am Soc Nephrol. 1995;6:177–183. - PubMed
-
- Charytan C, Spinowitz BS, Galler M. A comparative study of continuous ambulatory peritoneal dialysis and center hemodialysis. Efficacy, complications, and outcome in the treatment of end-stage renal disease. Arch Intern Med. 1986;146:1138–1143. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
