

Management of bleeding following major trauma: a European guideline
- PMID: 17298665
- PMCID: PMC2151863
- DOI: 10.1186/cc5686
Management of bleeding following major trauma: a European guideline
Erratum in
- Crit Care. 2007 Apr 24;11(2):414
Abstract
Introduction: Evidence-based recommendations can be made with respect to many aspects of the acute management of the bleeding trauma patient, which when implemented may lead to improved patient outcomes.
Methods: The multidisciplinary Task Force for Advanced Bleeding Care in Trauma was formed in 2005 with the aim of developing guidelines for the management of bleeding following severe injury. Recommendations were formulated using a nominal group process and the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) hierarchy of evidence and were based on a systematic review of published literature.
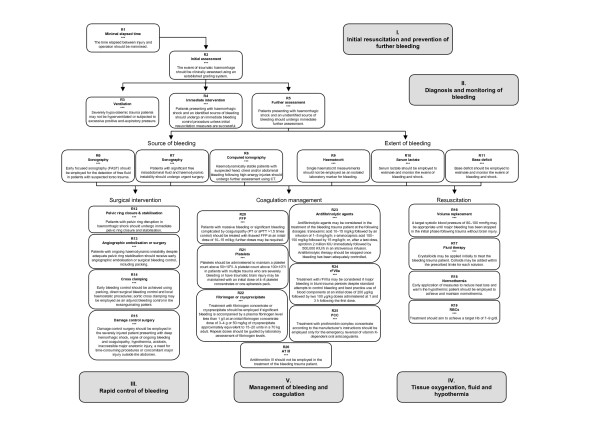
Results: Key recommendations include the following: The time elapsed between injury and operation should be minimised for patients in need of urgent surgical bleeding control, and patients presenting with haemorrhagic shock and an identified source of bleeding should undergo immediate surgical bleeding control unless initial resuscitation measures are successful. A damage control surgical approach is essential in the severely injured patient. Pelvic ring disruptions should be closed and stabilised, followed by appropriate angiographic embolisation or surgical bleeding control, including packing. Patients presenting with haemorrhagic shock and an unidentified source of bleeding should undergo immediate further assessment as appropriate using focused sonography, computed tomography, serum lactate, and/or base deficit measurements. This guideline also reviews appropriate physiological targets and suggested use and dosing of blood products, pharmacological agents, and coagulation factor replacement in the bleeding trauma patient.
Conclusion: A multidisciplinary approach to the management of the bleeding trauma patient will help create circumstances in which optimal care can be provided. By their very nature, these guidelines reflect the current state-of-the-art and will need to be updated and revised as important new evidence becomes available.
Figures
Comment in
-
Evidence-based guidelines for bleeding in trauma patients: where do we go from here?Crit Care. 2007;11(2):128. doi: 10.1186/cc5737. Crit Care. 2007. PMID: 17477884 Free PMC article.
References
-
- Krug E, Dahlberg L, Zwi A, Mercy J, Lozano R. World Report on Violence and Health. Geneva: World Health Organization; 2002. http://www.who.int/violence_injury_prevention/violence/world_report/en/
-
- Sauaia A, Moore FA, Moore EE, Moser KS, Brennan R, Read RA, Pons PT. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38:185–193. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
