

The potential of targeted antibody prophylaxis in SARS outbreak control: a mathematic analysis
- PMID: 17298911
- PMCID: PMC7106269
- DOI: 10.1016/j.tmaid.2006.01.007
The potential of targeted antibody prophylaxis in SARS outbreak control: a mathematic analysis
Abstract
Background: Severe acute respiratory syndrome (SARS) coronavirus-like viruses continue to circulate in animal reservoirs. If new mutants of SARS coronavirus do initiate another epidemic, administration of prophylactic antibodies to risk groups may supplement the stringent isolation procedures that contained the first SARS outbreak.
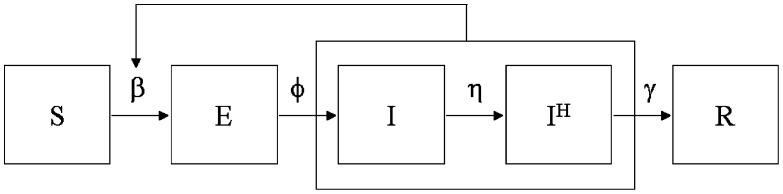
Method: We developed a mathematical model to investigate the effects of hospital admission and targeted antibody prophylaxis on the reproduction number R, defined as the number of secondary cases generated by an index case, during different SARS outbreak scenarios.
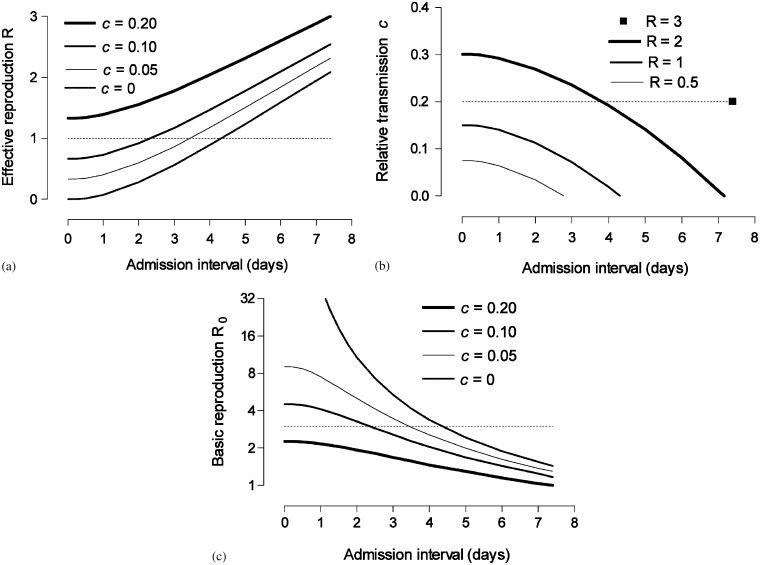
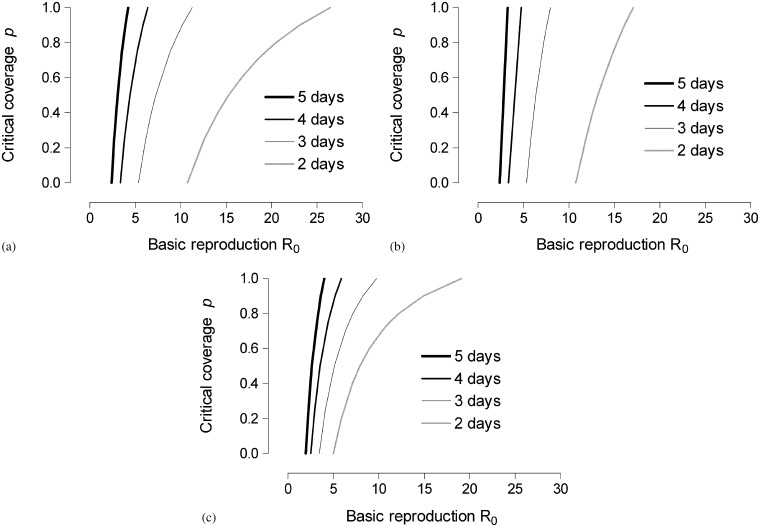
Results: Assuming a basic reproduction number R(0)=3, admission of patients to hospital within 4.3 days of symptom onset is necessary to achieve outbreak control without the need to further reduce community-based transmission. Control may be enhanced by providing pre-exposure prophylaxis to contacts of hospitalized patients, and through contact tracing and provision of post-exposure prophylaxis. Antibody prophylaxis may also be employed to reduce R below one and thereby restrict outbreak size and duration.
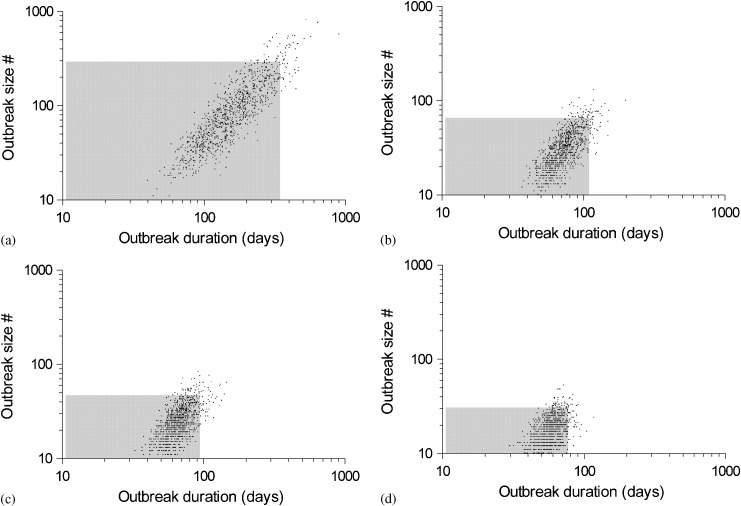
Conclusions: Patient isolation alone can be sufficient to control SARS outbreaks provided that the time from onset to admission is short. Antibody prophylaxis as supplemental measure generally allows for containment of higher R(0) values and restricts both the size and duration of an outbreak.
Figures
References
-
- World Health Organization. Consensus document on the epidemiology of severe acute respiratory syndrome (SARS). Geneva: Department of Communicable Disease Surveillance and Response, WHO; 2003.
-
- Riley S., Fraser C., Donnelly C.A., Ghani A.C., Abu-Raddad L.J., Hedley A.J. Transmission dynamics of the etiological agent of SARS in Hong Kong: impact of public health interventions. Science. 2003;300:1961–1966. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
