

A comparison of patients with relapsed and chemo-refractory gestational trophoblastic neoplasia
- PMID: 17299394
- PMCID: PMC2360082
- DOI: 10.1038/sj.bjc.6603608
A comparison of patients with relapsed and chemo-refractory gestational trophoblastic neoplasia
Abstract
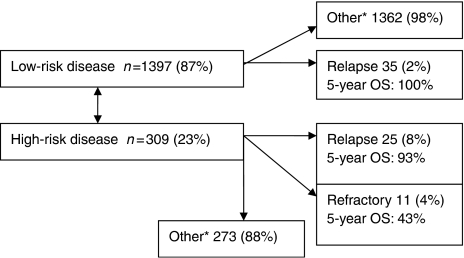
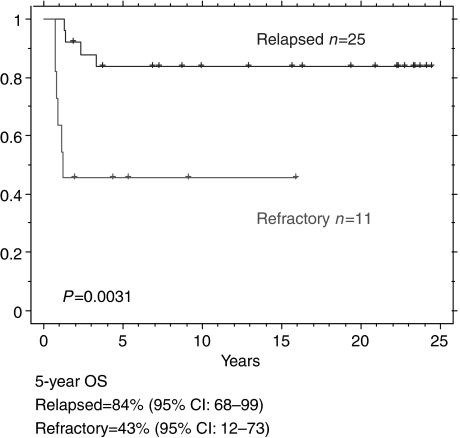
The majority of women requiring chemotherapy for gestational trophoblastic disease (GTN) are cured with their initial chemotherapy treatment. However, a small percentage either become refractory to treatment, or relapse after the completion of treatment. This study investigates the characteristics and outcome of these patients. Patients were identified from the Charing Cross Hospital GTD database. The outcome of these patients with relapsed disease was compared to those with refractory disease. Between 1980 and 2004, 1708 patients were treated with chemotherapy for GTN. Sixty (3.5%) patents relapsed following completion of initial therapy. The overall 5-year survival for patients with relapsed GTN was 93% (95% CI 86-100%). The overall survival for patients with low-risk and high-risk disease at presentation, who subsequently relapsed was 100% (n=35), and 84% (n=25) (95% CI: 66-96%: P<0.05), respectively. Eleven patients were identified who failed to enter remission and had refractory disease. These patients had a worse outcome compared to patients with relapsed disease (5-year survival 43% (95% CI:12-73% P<0.01)). The outcome of patients with relapsed GTN is good. However, patients with primary chemo-refractory disease do poorly and novel therapies are required for this group of patients.
Figures
References
-
- Bagshawe KD (1976) Risk and prognostic factors in trophoblastic neoplasia. Cancer 3: 1373–1385 - PubMed
-
- Bower M, Newlands ES, Holden L, Short D, Brock C, Rustin GJ, Begent RH, Bagshawe KD (1997) EMA/CO for high-risk gestational trophoblastic tumors: results from a cohort of 272 patients. J Clin Oncol 15: 2636–2643; Erratum in: J Clin Oncol 1997 September;15(9):3168. - PubMed
-
- Dobson LS, Lorigan PC, Coleman RE, Hancock BW (2000) Persistent gestational trophoblastic disease: results of MEA (methotrexate, etoposide and dactinomycin) as first-line chemotherapy in high risk disease and EA (etoposide and dactinomycin) as second-line therapy for low risk disease. Br J Cancer 82: 1547–1552 - PMC - PubMed
-
- Farhat F, Culine S, Theodore C, Bekradda M, Terrier-Lacombe MJ, Droz JP (1996) Cisplatin and ifosfamide with either vinblastine or etoposide as salvage therapy for refractory or relapsing germ cell tumor patients: the Institut Gustave Roussy experience. Cancer 77: 1193–1197 - PubMed
