

Findings from a buruli ulcer mouse model study
- PMID: 17299550
- PMCID: PMC1790819
Findings from a buruli ulcer mouse model study
Abstract
Summary introduction: Buruli ulcer disease is endemic in many developing countries in Africa. It is caused by Mycobacterium ulcerans, a toxin-producing bacterium with predilection for the skin and its deeper tissues. The exact mode of transmission is unclear and the pathogenesis is also not well understood, necessitating further elucidation through animal studies.
Objective: The study assessed the infectivity of a Ghanaian Mycobacterium ulcerans isolate and the dose-response pattern in BALB/c mice.
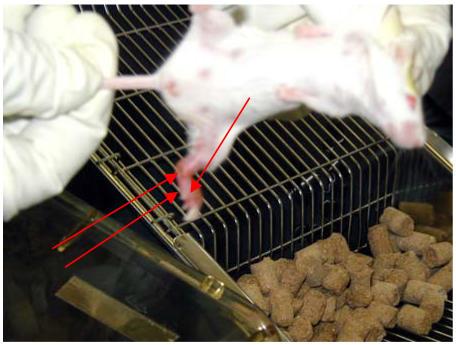
Method: Ten standardized bacterial suspensions of different concentrations were prepared from the M. ulcerans isolate and inoculated into the foot-pads of the mice. Thereafter they were observed for clinical signs of Buruli ulcer, upon which they were serially euthanised and evaluated for pathological and microbiological changes.
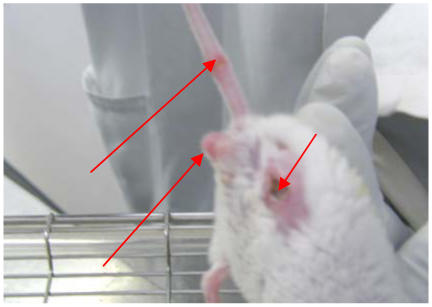
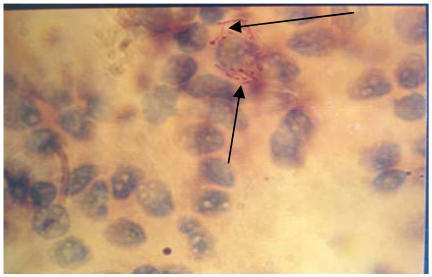
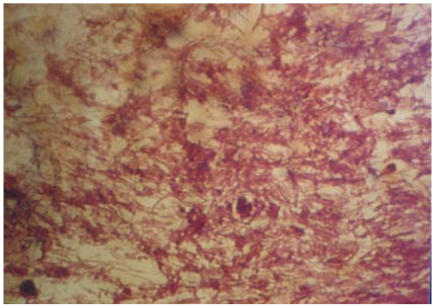
Results: Irrespective of the inoculum dose, all the experimentally infected mice developed similar clinical lesions, from erythema to foot ulceration (3.1 to 6.7 weeks after inoculation). However, the higher the inoculum dose the earlier the onset of the lesions. After the development of foot ulceration, mice that had received between 1 to 4 doses developed gangrene (5.7 to 7.2 weeks after inoculation) and died within a week, while those that had received 5 to 10 doses lost their limbs spontaneously (5.6 to 6.1 weeks after inoculation), followed by sudden clinical recovery. Eight weeks after the spontaneous amputation the amputees relapsed with concomitant metastasis, anasarca and death. Acid-fast bacilli (AFBs) were detected in inoculated and non-inoculated limbs, tails, visceral organs, faecal pellets and caecal contents of the mice. The AFBs detected in the caecal samples were innumerable and unusually long. Though AFBs were consistently detected in lymph nodes they were never detected in blood samples.
Conclusion: The findings suggest that the progression and final outcome of an M. ulcerans infection maybe dose related. The unequivocal absence of AFBs in the blood, but their consistent presence in lymph nodes located in the lower limbs right up to the neck, suggests that the microbes are disseminated through the lymphatic system rather than through the blood.
Figures
References
-
- Meyers WM, Tignokpa N, Priuli GB, Portaels F. Mycobacterium ulcerans infection (Buruli ulcer): first reported patients in Togo. Br J Dermatol. 1996;134:1116–1121. - PubMed
-
- Kreig RE, Hockmeyer WT, Connor DH. Toxin of Mycobacterium ulcerans. Production and effects in guinea pig skin. Arch Dermatol. 1974;110:783–788. - PubMed
-
- World Health Organisation, author. Buruli ulcer. 2001. Fact Sheet No 199. Available online at: http://www.who.int/inf-fs/en/fact199.htm.
-
- Meyers WM. Mycobacterial infections of the skin. In: Seifert G, editor. Tropical dermatology. Heidelberg: Springer-Verlag; 1994.
LinkOut - more resources
Full Text Sources