

Influencing referral practice using feedback of adherence to NICE guidelines: a quality improvement report for dyspepsia
- PMID: 17301208
- PMCID: PMC2464912
- DOI: 10.1136/qshc.2006.019992
Influencing referral practice using feedback of adherence to NICE guidelines: a quality improvement report for dyspepsia
Abstract
Problem: Rising demand and increasing waiting times for upper gastrointestinal endoscopy (gastroscopy).
Design: Quality improvement study with pre- and post-intervention data collection.
Setting: Three endoscopy units in two hospital trusts (Singleton, Morriston and Baglan Hospitals endoscopy units), UK.
Key measures for improvement: Number of gastroscopy requests from general practitioners (GPs) and hospital doctors; their adherence to dyspepsia referral guidelines and the referral-to-procedure interval for upper gastroscopy. Data collected for six months before and for five months after the intervention.
Strategy for change: Referrals were assessed against the National Institute for Health and Clinical Excellence (NICE) guidelines for the management of dyspepsia by two part-time GPs and feedback sent to clinicians where requests did not adhere to the referrals criteria
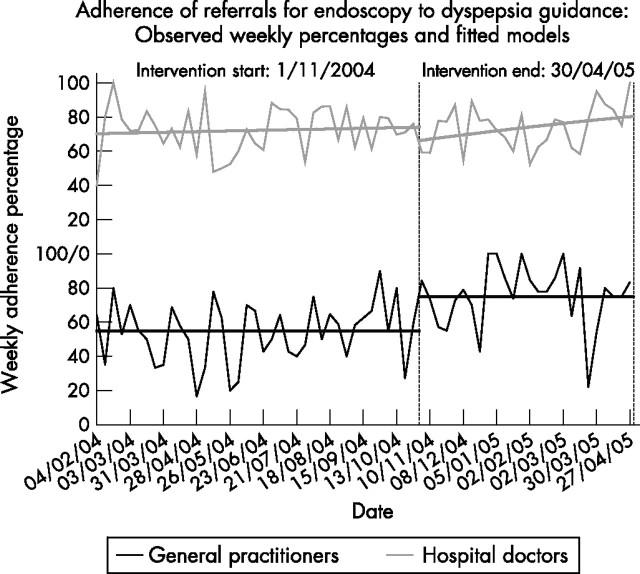
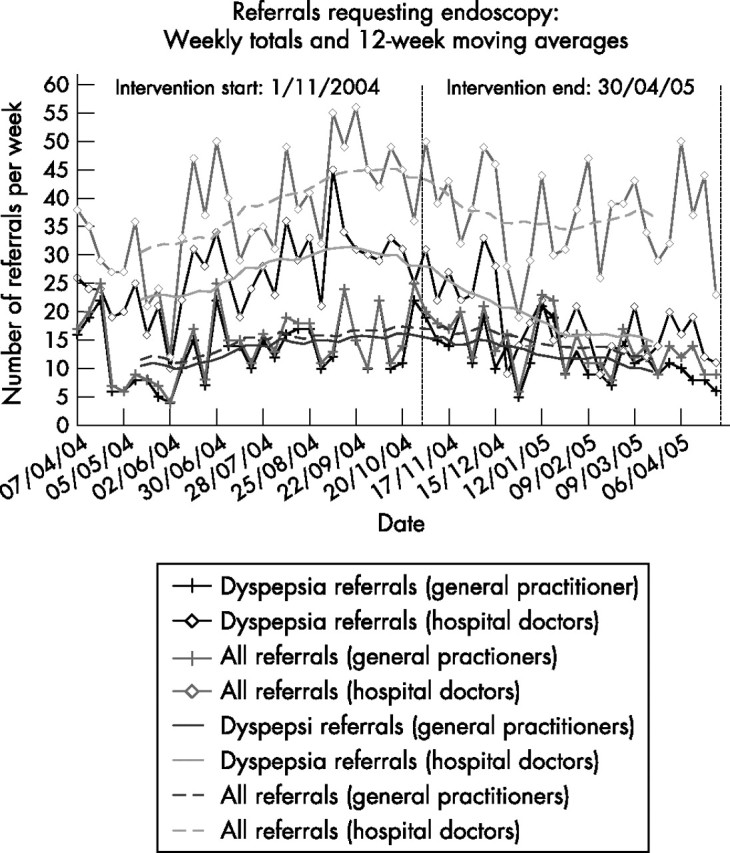
Effects of change: Adherence to guideline criteria increased significantly among GPs after the intervention (from 55% to 75%). There was no similar effect for hospital doctors, although their adherence rate (70%) was at a higher level than that of GPs before the intervention. The number of gastroscopy referrals for dyspepsia declined after the intervention, particularly from hospital doctors where a drop of 31% was observed, from 26.6 to 18.4 referrals per week. With the inclusion of seasonal effects, an estimated drop of 3.2 referrals per week from general practice was not significant (p = 0.065) while an estimated drop of 10.0 referrals per week for hospital doctors was very significant (p<0.001).
Lessons learnt: Referral assessment can be successfully introduced and shows promise as a way of improving the quality of referrals and reducing demand. Hospital clinicians are more resistant than GPs to referral assessment but nevertheless responded to the feedback by reducing their endoscopy gastroscopy requests. Most such referrals are generated in hospitals rather than in primary care: this finding has important implications for demand management.
Conflict of interest statement
Competing interests: None declared.
Similar articles
-
Reducing variation in general practitioner referral rates through clinical engagement and peer review of referrals: a service improvement project.Qual Prim Care. 2011;19(4):263-72. Qual Prim Care. 2011. PMID: 21902906
-
Pragmatic randomised controlled trial to evaluate guidelines for the management of infertility across the primary care-secondary care interface.BMJ. 2001 May 26;322(7297):1282-4. doi: 10.1136/bmj.322.7297.1282. BMJ. 2001. PMID: 11375232 Free PMC article. Clinical Trial.
-
Reducing community dyspepsia drug costs: a controlled trial.Gut. 2001 Oct;49(4):495-501. doi: 10.1136/gut.49.4.495. Gut. 2001. PMID: 11559645 Free PMC article. Clinical Trial.
-
Prevention of overuse: A view on upper gastrointestinal endoscopy.World J Gastroenterol. 2019 Jan 14;25(2):178-189. doi: 10.3748/wjg.v25.i2.178. World J Gastroenterol. 2019. PMID: 30670908 Free PMC article. Review.
-
Current guidelines for dyspepsia management.Dig Dis. 2008;26(3):225-30. doi: 10.1159/000121351. Epub 2008 May 6. Dig Dis. 2008. PMID: 18463440 Review.
Cited by
-
Improving quality of referral letters from primary to secondary care: a literature review and discussion paper.Prim Health Care Res Dev. 2018 May;19(3):211-222. doi: 10.1017/S1463423617000755. Epub 2017 Dec 7. Prim Health Care Res Dev. 2018. PMID: 29212565 Free PMC article. Review.
-
Guideline Adherence in Dyspepsia Investigation and Treatment.Kans J Med. 2020 Dec 11;13:306-310. doi: 10.17161/kjm.vol13.13838. eCollection 2020. Kans J Med. 2020. PMID: 33343824 Free PMC article.
-
Gastroscopy for dyspepsia: Understanding primary care and gastroenterologist mental models of practice: A cognitive task analysis approach.J Can Assoc Gastroenterol. 2023 Sep 27;6(6):234-243. doi: 10.1093/jcag/gwad035. eCollection 2023 Dec. J Can Assoc Gastroenterol. 2023. PMID: 38106487 Free PMC article.
-
Quality of referrals for elective surgery at a tertiary care hospital in a developing country: an opportunity for improving timely access to and cost-effectiveness of surgical care.Int J Surg. 2015 Mar;15:74-8. doi: 10.1016/j.ijsu.2015.01.033. Epub 2015 Feb 4. Int J Surg. 2015. PMID: 25659222 Free PMC article.
-
Overtesting and undertesting in primary care: a systematic review and meta-analysis.BMJ Open. 2018 Feb 11;8(2):e018557. doi: 10.1136/bmjopen-2017-018557. BMJ Open. 2018. PMID: 29440142 Free PMC article.
References
-
- National Endoscopy Team Improving endoscopy services. Leicester: National Endoscopy Team, 2005, Available at http://www.endoscopy.nhs.uk/resources/publications/Meeting%20the%20Chall... (accessed December 2006)
-
- NICE Dyspepsia: managing dyspesia in adults in primary care. London: National Institute for Health and Clinical Excellence, 2004
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials