

Pioglitazone improves insulin action and normalizes menstrual cycles in a majority of prenatally androgenized female rhesus monkeys
- PMID: 17306503
- PMCID: PMC2705750
- DOI: 10.1016/j.reprotox.2006.12.009
Pioglitazone improves insulin action and normalizes menstrual cycles in a majority of prenatally androgenized female rhesus monkeys
Abstract
Purpose of the study: To determine whether pioglitazone will improve menstrual cyclicity in a fetal programming model for polycystic ovary syndrome.
Basic procedures: Eight prenatally androgenized (PA) and 5 control female rhesus monkeys of similar age, body weight and body mass index received an oral placebo daily for 6-7 months followed, after at least 90 days, by daily oral dosing with pioglitazone (3mg/kg) for an additional 6-7 months. Blood was sampled thrice weekly to monitor ovulatory function, and a variety of endocrine challenges were performed to quantify changes in ovarian, gonadotropin and glucoregulatory function.
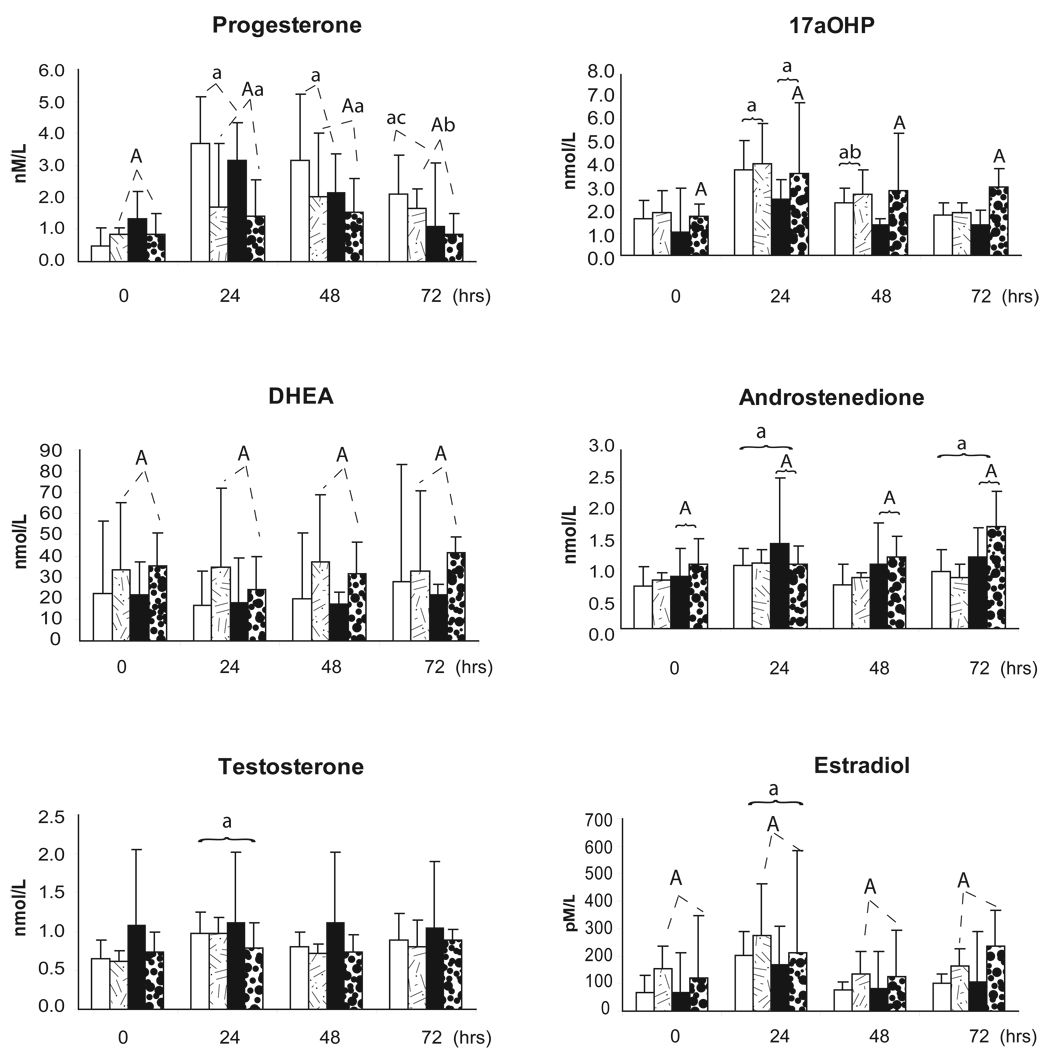
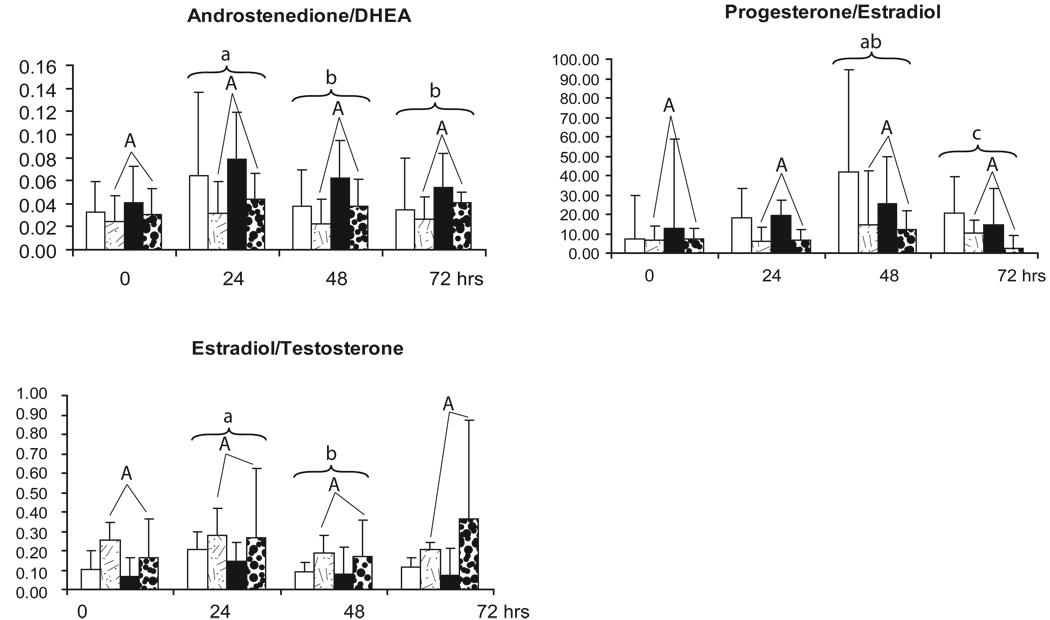
Most important findings: Pioglitazone normalized menstrual cycles in 5 out of 8 (62%) PA females (pioglitazone responsive; Pio(RESP)). Pioglitazone increased serum 17alpha-hydroxyprogesterone responses to an hCG injection in Pio(RESP) PA females, while diminishing serum progesterone, and increasing DHEA and estradiol responses to hCG in Pio(RESP) PA and all normal females.
Principal conclusions: Insulin resistance plays a mechanistic role in maintaining anovulation in a majority of PA female monkeys.
Figures

References
-
- Barnes RB, Rosenfield RL, Ehrmann DA, Cara JF, Cuttler L, Levitsky LL, Rosenthal IM. Ovarian hyperandrogynism as a result of congenital adrenal virilizing disorders: evidence for perinatal masculinization of neuroendocrine function in women. J Clin Endocrinol Metab. 1994;79:1328–1333. - PubMed
-
- Abbott DH, Dumesic DA, Franks S. Developmental origin of polycystic ovary syndrome - a hypothesis. J Endocrinol. 2002;174:1–5. - PubMed
-
- Xita N, Tsatsoulis A. Review: fetal programming of polycystic ovary syndrome by androgen excess: evidence from experimental, clinical, and genetic association studies. J Clin Endocrinol Metab. 2006;91:1660–1666. - PubMed
-
- Abbott DH, Dumesic DA, Eisner JR, Kemnitz JW, Goy RW. The prenatally androgenized female rhesus monkey as a model for polycystic ovarian syndrome. In: Dewailly D, editor. Androgen Excess Disorder in Women. Philadelphia, PA: Lippincot-Raven Press; 1997. pp. 369–382.
-
- Abbott DH, Dumesic DA, Eisner JR, Colman RJ, Kemnitz JW. Insights into the development of PCOS from studies of prenatally androgenized female rhesus monkeys. Trends Endocrinol Metab. 1998;9:62–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
