

Temporal trends in the treatment of pediatric type 1 diabetes and impact on acute outcomes
- PMID: 17307546
- PMCID: PMC1857326
- DOI: 10.1016/j.jpeds.2006.12.009
Temporal trends in the treatment of pediatric type 1 diabetes and impact on acute outcomes
Abstract
Objective: To evaluate temporal trends in pediatric type 1 diabetes (T1DM) management and resultant effects on outcomes.
Study design: Two pediatric T1DM cohorts were followed prospectively for 2 years and compared; Cohort 1 (N = 299) was enrolled in 1997 and Cohort 2 (N = 152) was enrolled in 2002. In both cohorts, eligible participants were identified and sequentially approached at regularly scheduled clinic visits until the target number of participants was reached. Main outcome measures were hemoglobin A1c (A1c), body mass index Z score (Z-BMI), and incidence rate (IR; per 100 patient-years) of hypoglycemia, hospitalizations, and emergency room (ER) visits.
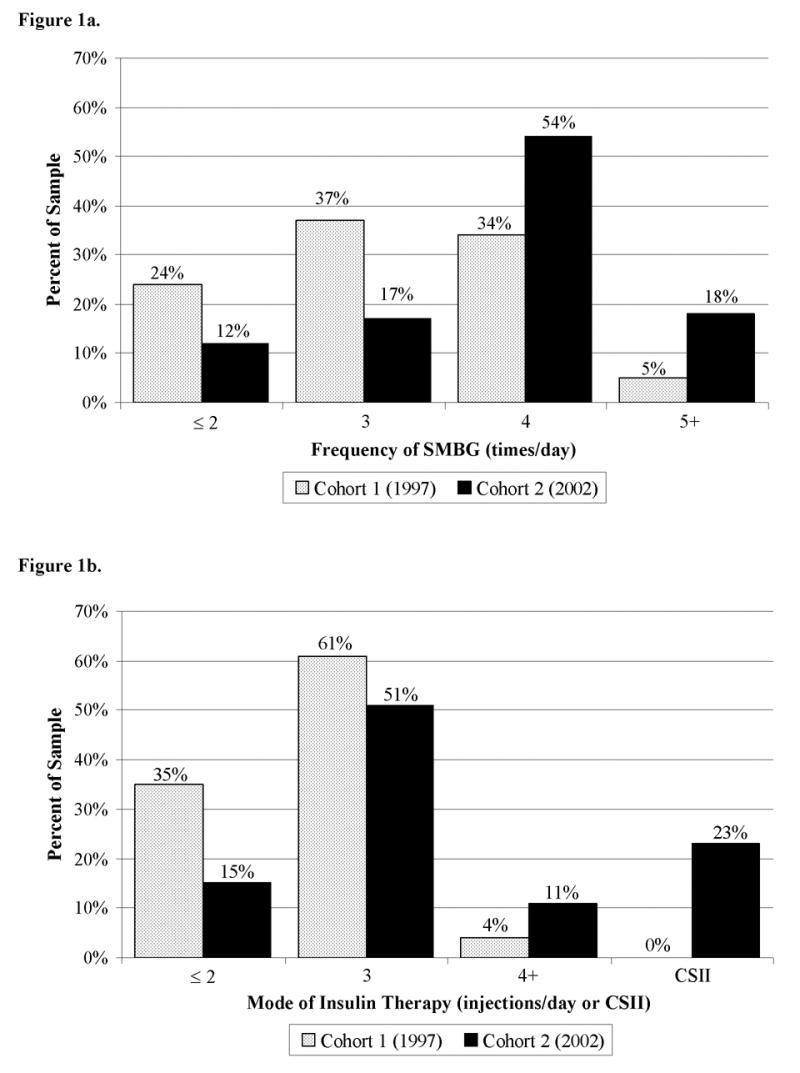
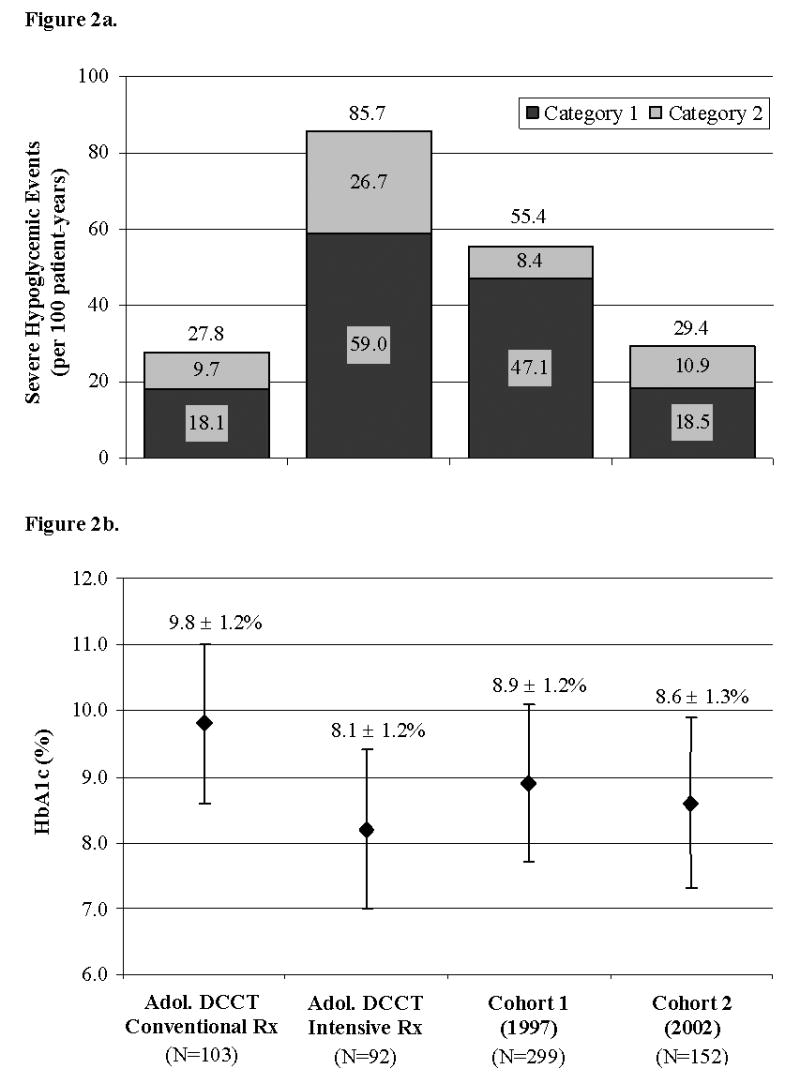
Results: At baseline, Cohort 2 monitored blood glucose more frequently than Cohort 1 (> or = 4 times/day: 72% vs 39%, P < .001) and was prescribed more intensive therapy than Cohort 1 (> or = 3 injections/day or pump: 85% vs 65%, P < .001). A1c was lower in Cohort 2 than Cohort 1 at baseline (8.4% vs 8.7%, P = .03) and study's end (8.7% vs 9.0%, P = .04). The cohorts did not differ in Z-BMI (0.83 vs 0.79, P = .57) or IR of hospitalizations (11.2 vs 12.9, P = .38). Cohort 2 had lower IR of total severe hypoglycemic events (29.4 vs 55.4, P < .001) and ER visits (22.0 vs 29.3, P = .02).
Conclusions: T1DM management intensified during the 5 years between cohorts and was accompanied by improved A1c and stable Z-BMI. Along with improved control, IR of severe hypoglycemia and ER visits decreased by almost 50% and 25%, respectively.
Figures
Similar articles
-
Use of the Continuous Glucose Monitoring System to guide therapy in patients with insulin-treated diabetes: a randomized controlled trial.Mayo Clin Proc. 2004 Dec;79(12):1521-6. doi: 10.4065/79.12.1521. Mayo Clin Proc. 2004. PMID: 15595336 Clinical Trial.
-
Effect of sensor-augmented insulin pump therapy and automated insulin suspension vs standard insulin pump therapy on hypoglycemia in patients with type 1 diabetes: a randomized clinical trial.JAMA. 2013 Sep 25;310(12):1240-7. doi: 10.1001/jama.2013.277818. JAMA. 2013. PMID: 24065010 Clinical Trial.
-
A randomized, controlled trial comparing twice-a-day insulin glargine mixed with rapid-acting insulin analogs versus standard neutral protamine Hagedorn (NPH) therapy in newly diagnosed type 1 diabetes.Pediatrics. 2008 Mar;121(3):e466-72. doi: 10.1542/peds.2007-1679. Epub 2008 Feb 25. Pediatrics. 2008. PMID: 18299307 Clinical Trial.
-
Detection of hypoglycemia by children with type 1 diabetes 6 to 11 years of age and their parents.Pediatrics. 2008 Dec;122(6):1408-9; author reply 1409. doi: 10.1542/peds.2008-2329. Pediatrics. 2008. PMID: 19047266 No abstract available.
-
Type 1 diabetes mellitus in pediatrics.Pediatr Rev. 2008 Nov;29(11):374-84; quiz 385. doi: 10.1542/pir.29-11-374. Pediatr Rev. 2008. PMID: 18977856 Review. No abstract available.
Cited by
-
The impact of hypoglycemia on quality of life and related outcomes in children and adolescents with type 1 diabetes: A systematic review.PLoS One. 2021 Dec 2;16(12):e0260896. doi: 10.1371/journal.pone.0260896. eCollection 2021. PLoS One. 2021. PMID: 34855927 Free PMC article.
-
Hemoglobin A1c Levels and risk of severe hypoglycemia in children and young adults with type 1 diabetes from Germany and Austria: a trend analysis in a cohort of 37,539 patients between 1995 and 2012.PLoS Med. 2014 Oct 7;11(10):e1001742. doi: 10.1371/journal.pmed.1001742. eCollection 2014 Oct. PLoS Med. 2014. PMID: 25289645 Free PMC article.
-
Diabetes in Youth: A Global Perspective.Endocrinol Metab Clin North Am. 2021 Sep;50(3):491-512. doi: 10.1016/j.ecl.2021.05.007. Epub 2021 Jul 13. Endocrinol Metab Clin North Am. 2021. PMID: 34399958 Free PMC article. Review.
-
Improved metabolic control in children and adolescents with type 1 diabetes: a trend analysis using prospective multicenter data from Germany and Austria.Diabetes Care. 2012 Jan;35(1):80-6. doi: 10.2337/dc11-0993. Epub 2011 Nov 10. Diabetes Care. 2012. PMID: 22074726 Free PMC article.
-
Longitudinal trends in HbA1c patterns and association with outcomes: A systematic review.Diabetes Metab Res Rev. 2018 Sep;34(6):e3015. doi: 10.1002/dmrr.3015. Epub 2018 May 22. Diabetes Metab Res Rev. 2018. PMID: 29663623 Free PMC article.
References
-
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86. - PubMed
-
- Silverstein J, Klingensmith G, Copeland K, Plotnick L, Kaufman F, Laffel L, et al. Care of children and adolescents with type 1 diabetes: a statement of the American Diabetes Association. Diabetes Care. 2005;28:186–212. - PubMed
-
- Haller MJ, Stalvey MS, Silverstein JH. Predictors of control of diabetes: monitoring may be the key. J Pediatr. 2004;144:660–1. - PubMed
-
- Nathan DM, McKitrick C, Larkin M, Schaffran R, Singer DE. Glycemic control in diabetes mellitus: have changes in therapy made a difference? Am J Med. 1996;100:157–63. - PubMed
-
- Levine BS, Anderson BJ, Butler DA, Brackett J, Laffel L. Predictors of glycemic control and short-term adverse outcomes in youth with type 1 diabetes. J Pediatr. 2001;139:197–203. - PubMed
