

Decrease in growth hormone and insulin-like growth factor (IGF)-1 release and amelioration of acromegaly features after rosiglitazone treatment of type 2 diabetes mellitus a patient with acromegaly
- PMID: 17309144
- PMCID: PMC2080491
Decrease in growth hormone and insulin-like growth factor (IGF)-1 release and amelioration of acromegaly features after rosiglitazone treatment of type 2 diabetes mellitus a patient with acromegaly
Abstract
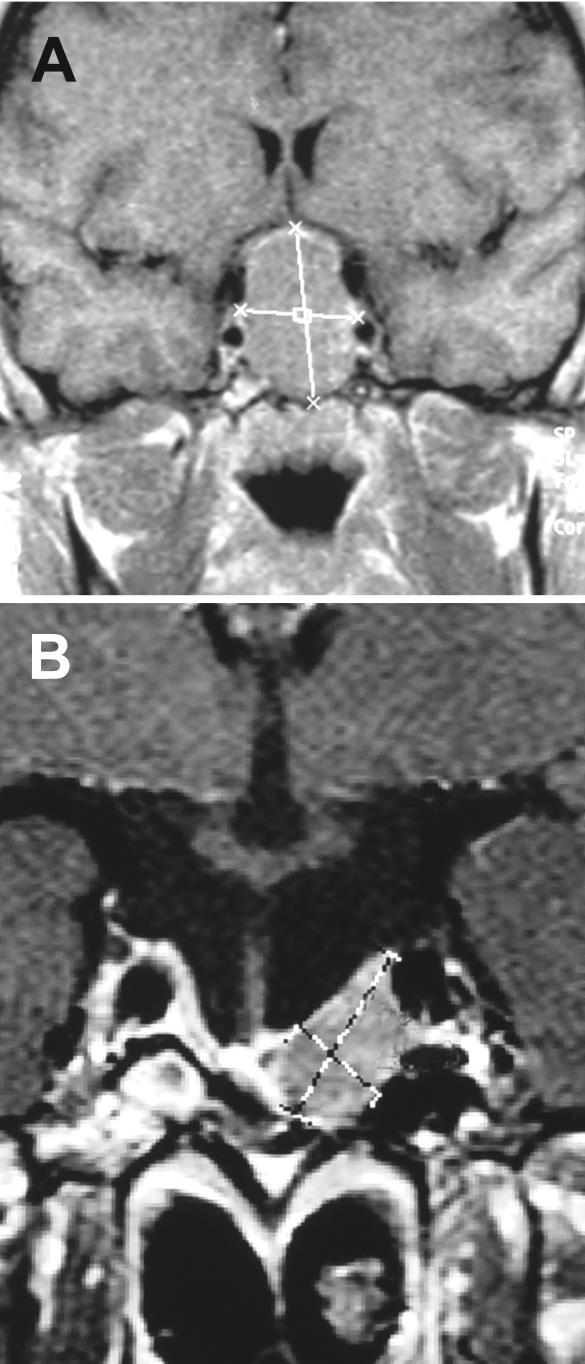
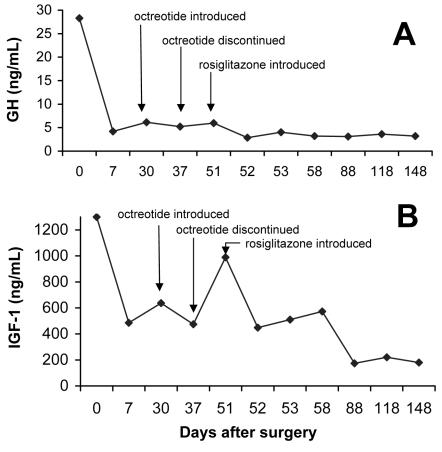
A 28-year-old woman with clinical features of acromegaly and diabetes mellitus was admitted to our Reference Center for Clinical Neuroendocrinology and Pituitary Diseases at Sisters of Mercy University Hospital, Zagreb, Croatia. Magnetic resonance scan of the brain showed pituitary macroadenoma. After transsphenoidal resection, histological analysis confirmed it was a growth hormone (GH)-secreting pituitary adenoma. The tumor could not be completely removed, but the hormonal status normalized. A month after the surgery, octreotide was introduced because of a further increase in GH and insulin-like growth factor-I (IGF-I), but discontinued after a week due to intolerance. Alternative treatment with oral antidiabetic agent, rosiglitazone, was introduced two weeks after octreotide was discontinued, and the fasting blood glucose concentration decreased from 8.4 mmol/L before the treatment to 6.7 mmol/L after 90 days of treatment. The concentration of GH and IGF-I in the week before rosiglitazone was introduced was 5.96 ng/mL and 990 ng/mL, respectively, and decreased to 2.92 ng/mL and 180.0 ng/mL, respectively, after 90 days of treatment. There was also a pronounced improvement in acromegalic features. It is possible that rosiglitazone induced the decrease in GH and IGF-I concentrations and its role in the long-term medical therapy of patients with pituitary tumors should be further investigated.
Figures
Similar articles
-
The PPAR-gamma activator rosiglitazone fails to lower plasma growth hormone and insulin-like growth factor-1 levels in patients with acromegaly.Neuroendocrinology. 2007;86(2):119-23. doi: 10.1159/000106830. Epub 2007 Aug 2. Neuroendocrinology. 2007. PMID: 17671378 Clinical Trial.
-
A prospective analysis of 151 cases of patients with acromegaly operated by one neurosurgeon: a follow-up of more than 23 years.Surg Neurol. 2006 Jul;66(1):26-31; discussion 31. doi: 10.1016/j.surneu.2005.11.063. Surg Neurol. 2006. PMID: 16793431
-
First-line octreotide-LAR therapy induces tumour shrinkage and controls hormone excess in patients with acromegaly: results from an open, prospective, multicentre trial.Clin Endocrinol (Oxf). 2006 Mar;64(3):342-51. doi: 10.1111/j.1365-2265.2006.02467.x. Clin Endocrinol (Oxf). 2006. PMID: 16487447
-
Hormonal diagnosis of GH hypersecretory states.J Endocrinol Invest. 2003;26(10 Suppl):27-35. J Endocrinol Invest. 2003. PMID: 15497657 Review.
-
Secondary diabetes associated with principal endocrinopathies: the impact of new treatment modalities.Acta Diabetol. 2009 Jun;46(2):85-95. doi: 10.1007/s00592-009-0112-9. Epub 2009 Mar 26. Acta Diabetol. 2009. PMID: 19322513 Review.
Cited by
-
Secondary diabetes mellitus in acromegaly.Endocrine. 2023 Jul;81(1):1-15. doi: 10.1007/s12020-023-03339-1. Epub 2023 Mar 8. Endocrine. 2023. PMID: 36882643 Free PMC article. Review.
-
Treatment of acromegaly by rosiglitazone via upregulating 15-PGDH in both pituitary adenoma and liver.iScience. 2021 Aug 14;24(9):102983. doi: 10.1016/j.isci.2021.102983. eCollection 2021 Sep 24. iScience. 2021. PMID: 34485865 Free PMC article.
-
Assessing the benefits of rosiglitazone in women with polycystic ovary syndrome through its effects on insulin-like growth factor 1, insulin-like growth factor-binding protein-3 and insulin resistance: a pilot study.Clinics (Sao Paulo). 2012;67(3):283-7. doi: 10.6061/clinics/2012(03)14. Clinics (Sao Paulo). 2012. PMID: 22473412 Free PMC article. Clinical Trial. No abstract available.
-
A case of fugitive acromegaly, initially presented as invasive prolactinoma.Endocrine. 2010 Aug;38(1):1-5. doi: 10.1007/s12020-010-9341-5. Epub 2010 Apr 24. Endocrine. 2010. PMID: 20960094
-
Bone loss in diabetes: use of antidiabetic thiazolidinediones and secondary osteoporosis.Curr Osteoporos Rep. 2010 Dec;8(4):178-84. doi: 10.1007/s11914-010-0027-y. Curr Osteoporos Rep. 2010. PMID: 20809203 Free PMC article. Review.
References
-
- Katznelson L. Diagnosis and treatment of acromegaly. Growth Horm IGF Res. 2005;15 Suppl A:S31–5. - PubMed
-
- Giustina A, Barkan A, Casanueva FF, Cavagnini F, Frohman L, Ho KJ, et al. Criteria for cure of acromegaly: a consensus statement. J Clin Endocrinol Metab. 2000;85:526–9. - PubMed
-
- Jones JI, Clemmons DR. Insulin-like growth factors and their binding proteins: biological actions. Endocr Rev. 1995;16:3–26. - PubMed
-
- Frohman LA. Acromegaly: what constitutes optimal therapy? J Clin Endocrinol Metab. 1996;81:443–5. - PubMed
-
- Wass JA, Shalet SM, editors. Oxford textbook of endocrinology. 1st ed. Oxford: Oxford University Press; 2002.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous