

Dual-head lithotripsy in synchronous mode: acute effect on renal function and morphology in the pig
- PMID: 17309558
- PMCID: PMC2529163
- DOI: 10.1111/j.1464-410X.2006.06736.x
Dual-head lithotripsy in synchronous mode: acute effect on renal function and morphology in the pig
Abstract
Objective: To assess the effect of dual-head lithotripsy on renal function and morphology in a pig model of shockwave (SW) injury, as lithotripters with two shock heads are now available for treating patients, but little information is available with which to judge the safety of treatment with dual pulses.
Materials and methods: A dual-head electrohydraulic lithotripter (Duet, Direx Corp., Natick, MA, USA) was used to treat the lower renal pole of anaesthetized pigs with a clinical dose of SWs (2400 dual SWs; 10 kidneys) delivered in synchronous mode, i.e. both heads fired simultaneously. For comparison, pigs were treated with either 2400 SWs (12 kidneys) or 4800 SWs (eight) with a conventional electrohydraulic lithotripter (HM3, Dornier, Wessling, Germany).
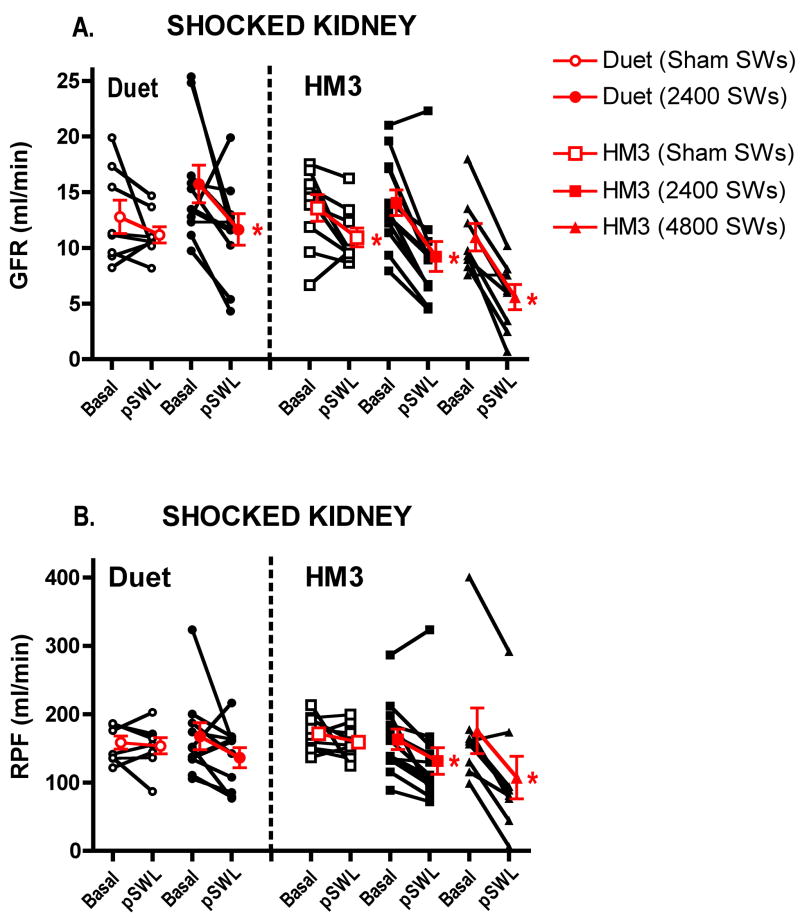
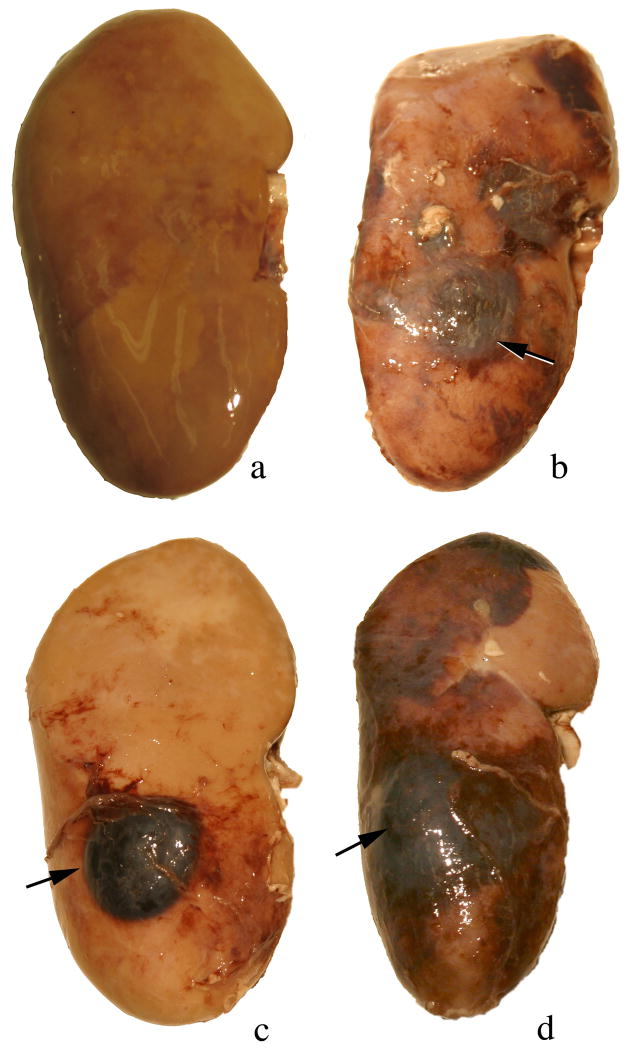
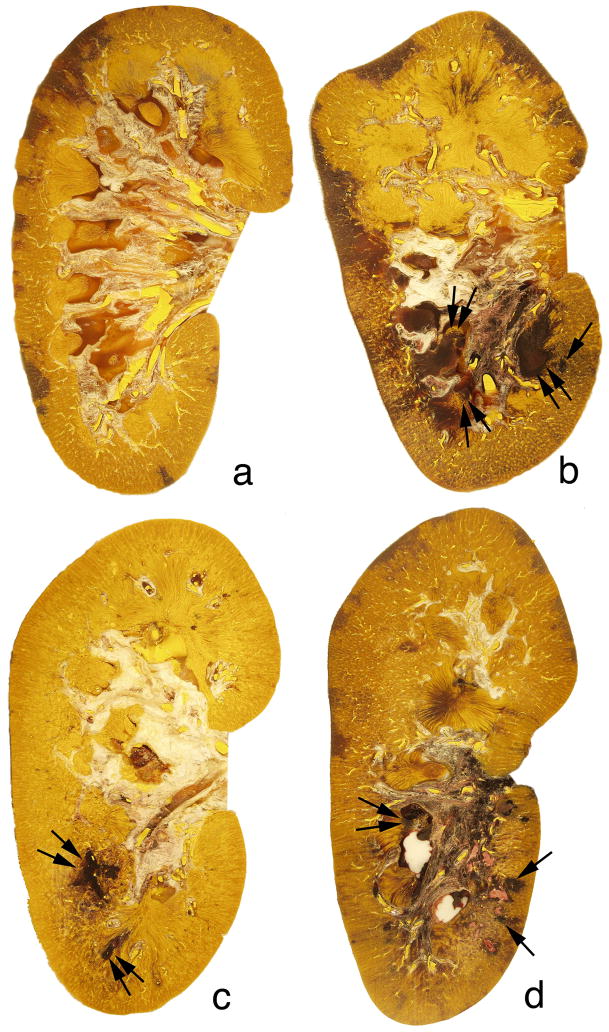
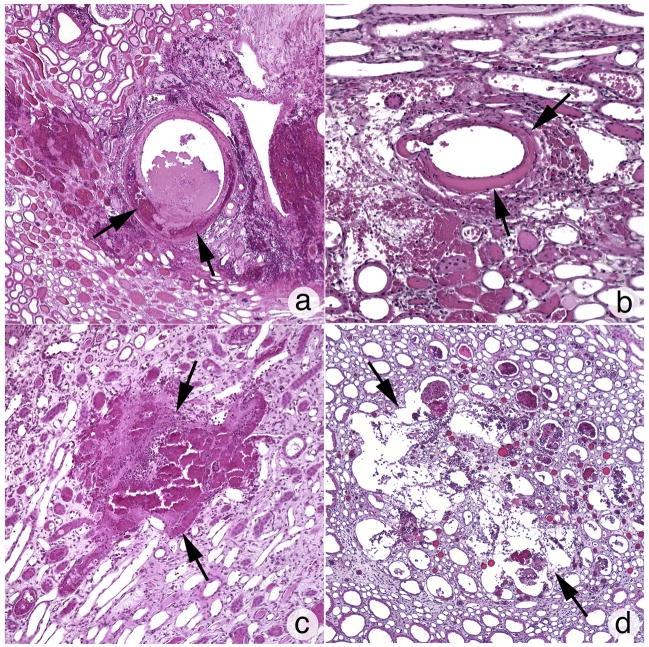
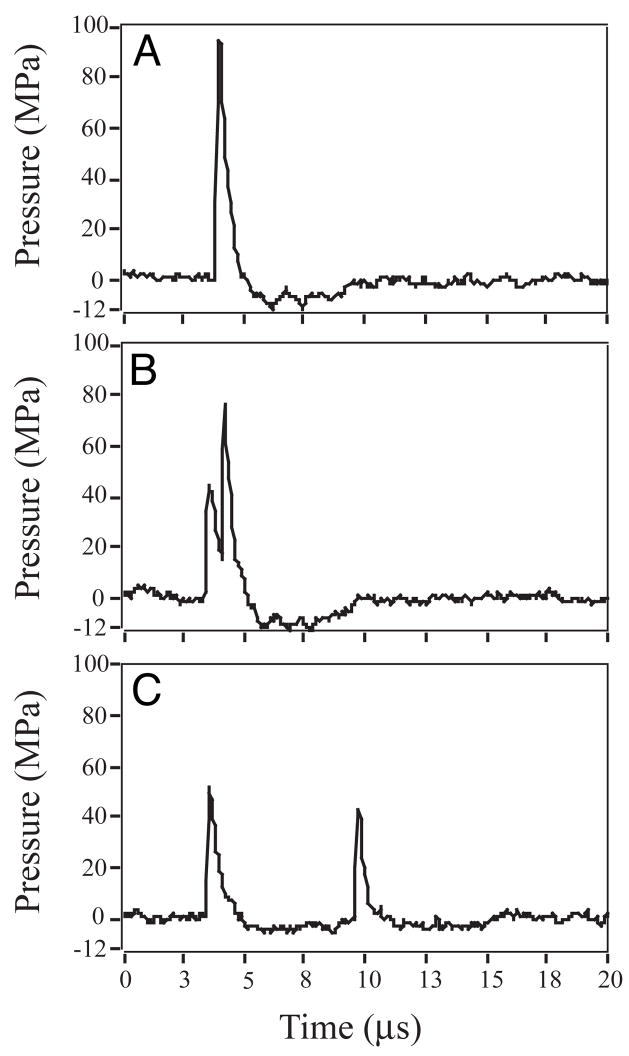
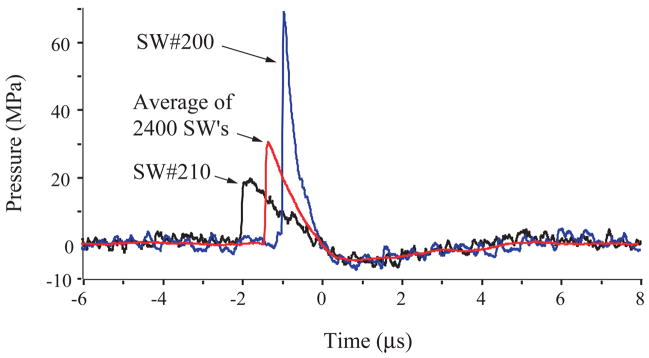
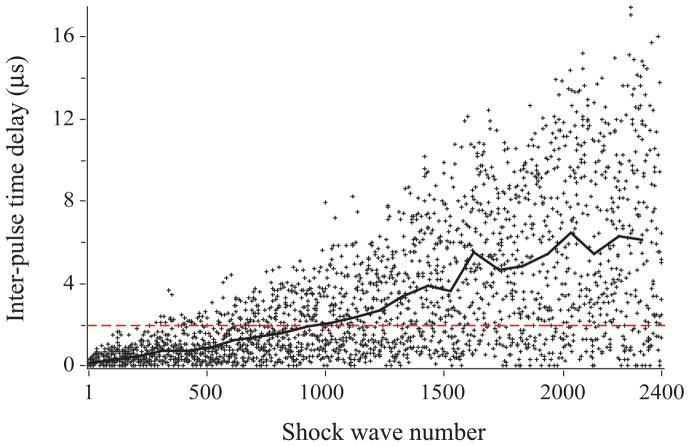
Results: Dual-pulse SW treatment with the Duet lithotripter caused a decline in the mean (sd) glomerular filtration rate (GFR) of 4.1 (1.9) mL/min, with a trend for the effective renal plasma flow (RPF), at 31 (19) mL/min, to also decrease. These changes in renal haemodynamics were similar to the decreases in GFR and RPF in response to treatment with the HM3 lithotripter with 2400 SWs, at 4.8 (0.8) and 32 (10) mL/min, respectively, or 4800 SWs, at 5.4 (1.0) and 68 (14) mL/min, respectively. Linear association analysis showed that the functional response to dual-pulse SWs was more variable than with conventional SWs. Morphological quantification of kidney damage (expressed as a percentage of functional renal volume, FRV) showed that tissue injury with 2400 paired SWs with the Duet, at 0.96 (0.39)% FRV, was similar to injury produced by either 2400 single SWs, at 1.08 (0.38)% FRV, or 4800 single SWs, at 2.71 (1.02)% FRV, with the HM3. However, morphological damage was less consistent with the Duet (measurable in only five of eight kidneys) than that with the HM3 (measurable in all 12 kidneys). Acoustic output and the timing of dual SWs in synchronous mode increased in variability as the electrodes aged, affecting the amplitude and targeting of focal pressures.
Conclusion: With the caveat that variability in the timing of dual SWs will unpredictably alter the distribution of SW energy within the kidney, this study shows that a clinical dose of dual-head SWs delivered in synchronous mode elicits a renal response similar to, but more variable than, that with a clinical dose of SWs from a conventional electrohydraulic lithotripter.
Figures
Similar articles
-
Evaluation of shock wave lithotripsy injury in the pig using a narrow focal zone lithotriptor.BJU Int. 2012 Nov;110(9):1376-85. doi: 10.1111/j.1464-410X.2012.11160.x. Epub 2012 Apr 23. BJU Int. 2012. PMID: 22519983 Free PMC article.
-
Independent assessment of a wide-focus, low-pressure electromagnetic lithotripter: absence of renal bioeffects in the pig.BJU Int. 2008 Feb;101(3):382-8. doi: 10.1111/j.1464-410X.2007.07231.x. Epub 2007 Oct 8. BJU Int. 2008. PMID: 17922871
-
Optimising an escalating shockwave amplitude treatment strategy to protect the kidney from injury during shockwave lithotripsy.BJU Int. 2012 Dec;110(11 Pt C):E1041-7. doi: 10.1111/j.1464-410X.2012.11207.x. Epub 2012 May 22. BJU Int. 2012. PMID: 22612388 Free PMC article.
-
Treatment protocols to reduce renal injury during shock wave lithotripsy.Curr Opin Urol. 2009 Mar;19(2):192-5. doi: 10.1097/mou.0b013e32831e16e3. Curr Opin Urol. 2009. PMID: 19195131 Free PMC article. Review.
-
Update on shock wave lithotripsy technology.Curr Opin Urol. 2002 Jul;12(4):287-90. doi: 10.1097/00042307-200207000-00005. Curr Opin Urol. 2002. PMID: 12072648 Review.
Cited by
-
Experimental observations and numerical modeling of lipid-shell microbubbles with calcium-adhering moieties for minimally-invasive treatment of urinary stones.Proc Meet Acoust. 2018;35(1):020008. doi: 10.1121/2.0000958. Epub 2019 Jan 17. Proc Meet Acoust. 2018. PMID: 32440311 Free PMC article.
-
Novel instrumentation in urologic surgery: Shock wave lithotripsy.Indian J Urol. 2010 Jul;26(3):423-6. doi: 10.4103/0970-1591.70780. Indian J Urol. 2010. PMID: 21116366 Free PMC article.
-
Evaluation of shock wave lithotripsy injury in the pig using a narrow focal zone lithotriptor.BJU Int. 2012 Nov;110(9):1376-85. doi: 10.1111/j.1464-410X.2012.11160.x. Epub 2012 Apr 23. BJU Int. 2012. PMID: 22519983 Free PMC article.
-
Assessment of renal injury with a clinical dual head lithotriptor delivering 240 shock waves per minute.J Urol. 2009 Feb;181(2):884-9. doi: 10.1016/j.juro.2008.10.065. Epub 2008 Dec 17. J Urol. 2009. PMID: 19095269 Free PMC article.
-
Comparison of tissue injury from focused ultrasonic propulsion of kidney stones versus extracorporeal shock wave lithotripsy.J Urol. 2014 Jan;191(1):235-41. doi: 10.1016/j.juro.2013.07.087. Epub 2013 Aug 2. J Urol. 2014. PMID: 23917165 Free PMC article.
References
-
- Lingeman JE. Lithotripsy systems. In: Smith AD, Badlani GH, Bagley DH, Clayman RV, Docimo SG, Jordan GH, Kavoussi LR, Lee BR, Lingeman JE, Preminger GM, Segura JW, editors. Smith’s Textbook on Endourology. Hamilton, Ontario, Canada: BC Decker, Inc; 2007. pp. 333–42.
-
- Bailey MR. Control of acoustic cavitation with application to lithotripsy. University of Texas; Austin: 1997. [Ph.D. dissertation]
-
- Zhong P, Cocks FH, Cioanta I, Preminger GM. Controlled, forced collapse of cavitation bubbles for improved stone fragmentation during shock wave lithotripsy. J Urol. 1997;158:2323–8. - PubMed
-
- Huber P, Debus J, Jöchle K, et al. Control of cavitation activity by different shockwave pulsing regimes. Phys Med Biol. 1999;44:1427–37. - PubMed
-
- Loske AM, Fernandez F, Zendejas H, Paredes M, Castano-Tostado E. Dual pulse shock wave lithotripsy: in vitro and in vivo study. J Urol. 2005;174:2388–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
