

Improving end-of-life care for patients with chronic heart failure: "Let's hope it'll get better, when I know in my heart of hearts it won't"
- PMID: 17309905
- PMCID: PMC1994396
- DOI: 10.1136/hrt.2006.106518
Improving end-of-life care for patients with chronic heart failure: "Let's hope it'll get better, when I know in my heart of hearts it won't"
Abstract
Background: Although chronic heart failure (CHF) has a high mortality rate and symptom burden, and clinical guidance stipulates palliative care intervention, there is a lack of evidence to guide clinical practice for patients approaching the end of life.
Aims: (1) To formulate guidance and recommendations for improving end-of-life care in CHF; (2) to generate data on patients' and carers' preferences regarding future treatment modalities, and to investigate communication between staff, patients and carers on end-of-life issues.
Design: Semistructured qualitative interviews were conducted with 20 patients with CHF (New York Heart Association functional classification III-IV), 11 family carers, 6 palliative care clinicians and 6 cardiology clinicians.
Setting: A tertiary hospital in London, UK.
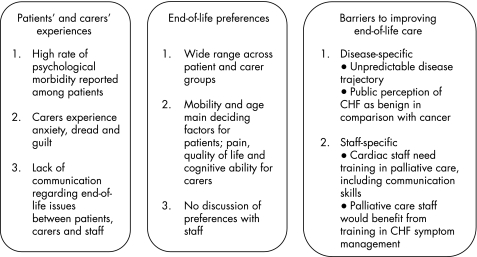
Results: Patients and families reported a wide range of end-of-life care preferences. None had discussed these with their clinicians, and none was aware of choices or alternatives in future care modalities, such as adopting a palliative approach. Patients and carers live with fear and anxiety, and are uninformed about the implications of their diagnosis. Cardiac staff confirmed that they rarely raise such issues with patients. Disease- and specialism-specific barriers to improving end-of-life care were identified.
Conclusions: The novel, integrated data presented here provide three recommendations for improving care in line with policy directives: sensitive provision of information and discussion of end-of-life issues with patients and families; mutual education of cardiology and palliative care staff; and mutually agreed palliative care referral criteria and care pathways for patients with CHF.
Conflict of interest statement
Competing interests: None.
Comment in
-
Improving end-of-life care for patients with chronic heart failure.Heart. 2007 Aug;93(8):901-2. doi: 10.1136/hrt.2006.109330. Heart. 2007. PMID: 17639106 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical