

Comparison of clinical and economic outcomes of two antibiotic prophylaxis regimens for sternal wound infection in high-risk patients following coronary artery bypass grafting surgery: a prospective randomised double-blind controlled trial
- PMID: 17309908
- PMCID: PMC1955036
- DOI: 10.1136/hrt.2006.103002
Comparison of clinical and economic outcomes of two antibiotic prophylaxis regimens for sternal wound infection in high-risk patients following coronary artery bypass grafting surgery: a prospective randomised double-blind controlled trial
Abstract
Objective: Prospective studies show a 10% incidence of sternal wound infection (SWI) after 90 days of follow-up, compared with infection rates of 5% reported by the National Nosocomial Infections Surveillance System after only 30 days of follow-up. This incidence increases 2-3 times in high-risk patients.
Design: Prospective randomised double-blind controlled clinical trial.
Setting: Cardiothoracic centre, UK.
Patients: Patients were eligible if they were undergoing median sternotomy for primary isolated coronary artery bypass grafting, with at least one internal thoracic artery used for coronary grafting and having one or more of the following three risk factors: (1) obesity, defined as body mass index 30 kg/m(2); (2) diabetes mellitus; or (3) bilateral internal thoracic artery grafts (ie, the use of the other internal thoracic artery).
Interventions: The study group received a single dose of gentamicin 2 mg/kg, rifampicin 600 mg and vancomycin 15 mg/kg, with three further doses of 7.5 mg/kg at 12-hour intervals. The control group received cefuroxime 1.5 g at induction and three further doses of 750 mg at 8-hour intervals.
Main outcome measures: The primary end point was the incidence of SWI at 90 days. The secondary end point was the antibiotic and hospital costs.
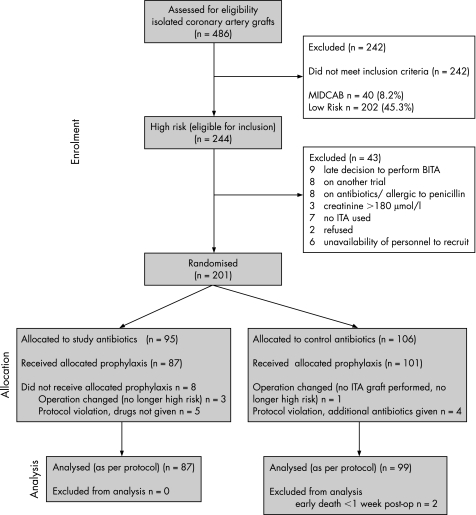
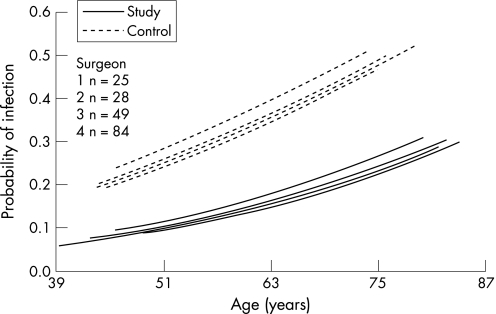
Results: During the study period, 486 patients underwent isolated coronary artery bypass grafting with a 30-day SWI of 7.6%. 186 high-risk patients were recruited and analysed: 87 in the study group and 99 in the control group. 90-day SWI was significantly reduced in 8 patients in the study group (9.2%; 95% CI 3.5% to 15.3%) compared with 25 patients in the control group (25.2%; 95% CI 19.5% to 39.4%; p = 0.004). The study group had a significantly lower cost of antibiotics (21.2% reduction--US$96/patient; p<0.001), and a significantly lower hospital cost (20.4% reduction in cost--US$3800/patient; p = 0.04).
Conclusions: Longer and broader-spectrum antibiotic prophylaxis significantly reduces the incidence of SWI in high-risk patients, with a significant economic benefit in costs of antibiotics as well as hospital costs.
Conflict of interest statement
Competing interests: None.
Comment in
-
Antibiotic prophylaxis in cardiac surgery.Heart. 2008 May;94(5):646; author reply 646. doi: 10.1136/hrt.2007.139188. Heart. 2008. PMID: 18411357 No abstract available.
References
-
- Milton H. Mediastinal surgery. Lancet 1897I872
-
- Kreter B, Woods M. Antibiotic prophylaxis for cardiothoracic operations. Meta‐analysis of thirty years of clinical trials. J Thorac Cardiovasc Surg 1992104590–599. - PubMed
-
- Ridderstolpe L, Gill H, Granfeldt H. Superficial and deep sternal wound complications: incidence, risk factors, and mortality. Eur J Cardiothorac Surg 2001201168–1175. - PubMed
-
- Jonkers D, Elenbaas T, Terporten P.et al Prevalence of 90‐days postoperative wound infections after cardiac surgery. Eur J Cardiothorac Surg 20032397–102. - PubMed
-
- Gummert J F, Barten M J, Hans C. Mediastinitis and cardiac surgery—an updated risk factor analysis in 10,373 consecutive adult patients. Thorac Cardiovasc Surg 20025087–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical