

Survival advantage with decitabine versus intensive chemotherapy in patients with higher risk myelodysplastic syndrome: comparison with historical experience
- PMID: 17315156
- PMCID: PMC2952542
- DOI: 10.1002/cncr.22508
Survival advantage with decitabine versus intensive chemotherapy in patients with higher risk myelodysplastic syndrome: comparison with historical experience
Abstract
Background: Decitabine, a hypomethylating agent, is active and has been approved for the treatment of myelodysplastic syndrome (MDS) and chronic myelomonocytic leukemia. Intensive chemotherapy is an accepted form of therapy for patients with higher risk MDS. The comparative efficacy of these 2 forms of treatment in MDS is unknown. The objective of the current study was to compare the efficacy and toxicity profiles of decitabine and intensive chemotherapy in MDS.
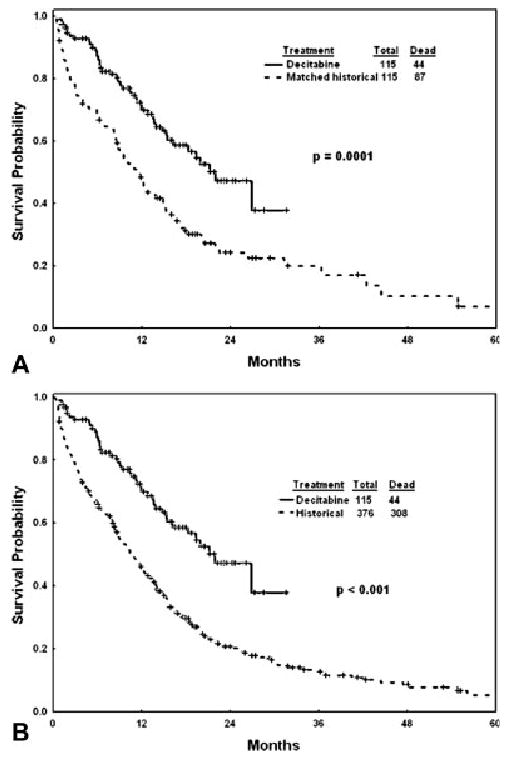
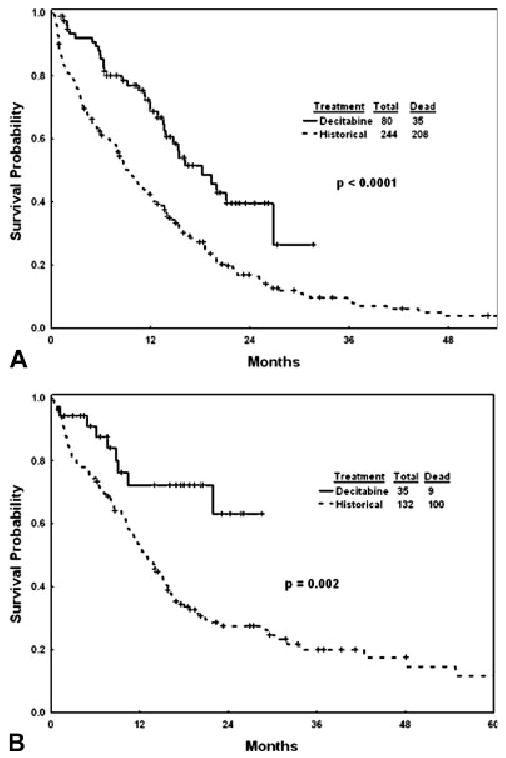
Methods: The authors compared lower intensity decitabine therapy (n = 115 patients) with intensive chemotherapy (as it is used in acute myeloid leukemia [AML]) in patients with higher risk MDS. Two comparisons were made with a cohort of 376 historic patients (from 1995 to 2005): The first comparison included a subcohort of 115 patients (Group A) who matched the 115 decitabine study patients according to age, International Prognostic Scoring System, and cytogenetics; and the second comparison included the whole cohort of 376 patients without matching (Group B). A multivariate analysis was performed for outcome.
Results: The complete remission (CR) rate according to AML criteria was 43% with decitabine, 46% with intensive chemotherapy in Group A, and 52% with intensive chemotherapy in Group B. Compared with Group A, mortality at 6 weeks was 3% with decitabine versus 13% with intensive chemotherapy (P = .006) and, at 3 months, 7% with decitabine versus 23% with intensive chemotherapy (P = .001). Survival was better with decitabine versus intensive chemotherapy in Group A (median survival: 22 months vs 12 months; P < .001). A multivariate analysis of survival in all 491 patients who received decitabine or intensive chemotherapy (Group B) selected decitabine as an independent, favorable prognostic factor for survival (P = .006; hazard ratio, 0.74) after accounting for the independent prognostic effect of pretreatment factors.
Conclusions: In this analysis, decitabine was associated with a survival advantage compared with intensive chemotherapy in patients with higher risk MDS. Future studies should evaluate prospectively the results of decitabine versus intensive chemotherapy in this setting.
Figures
References
-
- Faderl S, Kantarjian H. Novel therapies for myelodysplastic syndromes. Cancer. 2004;101:226–241. - PubMed
-
- Faderl S, Kantarjian H. Myelodysplastic syndromes. In: DeVita V, Hellman S, Rosenberg S, editors. Cancer: Principles and Practice of Oncology. 7th. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. pp. 2144–2154.
-
- Bennett JM, Catovsky D, Daniel MT, et al. Proposals for the classification of the myelodysplastic syndromes. Br J Haematol. 1982;51:189–199. - PubMed
-
- Harris NJ, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting, Airlie House, Virginia, November 1977. J Clin Oncol. 1999;17:3835–3849. - PubMed
-
- Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89:2079–2088. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
