

Review
doi: 10.1186/cc5668.
Clinical review: Bedside lung ultrasound in critical care practice
Affiliations
- PMID: 17316468
- PMCID: PMC2151891
- DOI: 10.1186/cc5668
Item in Clipboard
Review
Clinical review: Bedside lung ultrasound in critical care practice
Crit Care.
2007.
Abstract
Lung ultrasound can be routinely performed at the bedside by intensive care unit physicians and may provide accurate information on lung status with diagnostic and therapeutic relevance. This article reviews the performance of bedside lung ultrasound for diagnosing pleural effusion, pneumothorax, alveolar-interstitial syndrome, lung consolidation, pulmonary abscess and lung recruitment/derecruitment in critically ill patients with acute lung injury.
Figures

Ultrasound pattern of normal lung. The pleural line (white arrow) is a roughly horizontal hyperechoic line 0.5 cm below the upper and lower ribs identified by acoustic shadow (R). A single vertical artifact arising from the pleural line and spreading up to the edge of the screen (comet-tails, indicated by asterisk) can be seen in dependant regions in normally aerated lungs.
Ultrasound aspects of alveolar-interstitial syndrome. (a) B-lines 7 mm apart or spaced comet-tail artifacts. The pleural line (white arrow) and the ribs (R) with their acoustic shadow. Spaced comet-tail artifacts (indicated by asterisks) or B-lines arising from the pleural line and spreading up to the edge of the screen are present. These artifacts correspond to thickened interlobular septa on chest CT scan. (b) B-lines 3 mm or less apart. The pleural line (white arrow) and the rib (R) with their acoustic shadow. Contiguous comet-tails arising from the pleural line and spreading up to the edge of screen are present. These artefacts correspond to ground-glass areas on chest CT scan.
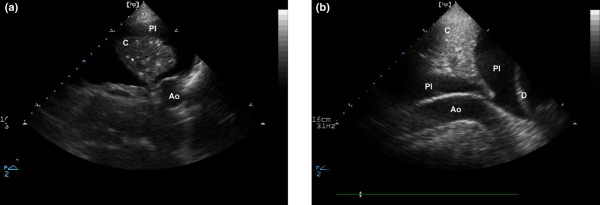
Ultrasound aspect of a lung consolidation and a pleural effusion. (a) Transversal view of consolidated left lower lobe; lung consolidation is seen as a tissular structure (C). In this consolidation, hyperechoic punctiform images (indicated by asterisk) can be seen; these correspond to air bronchograms (air-filled bronchi). Pleural effusion is anechoic (Pl). (b) Cephalocaudal view of consolidated left lower lobe: lung consolidation with air bronchograms. Ao, descending aorta; D, diaphragm; Pl, pleural effusion.
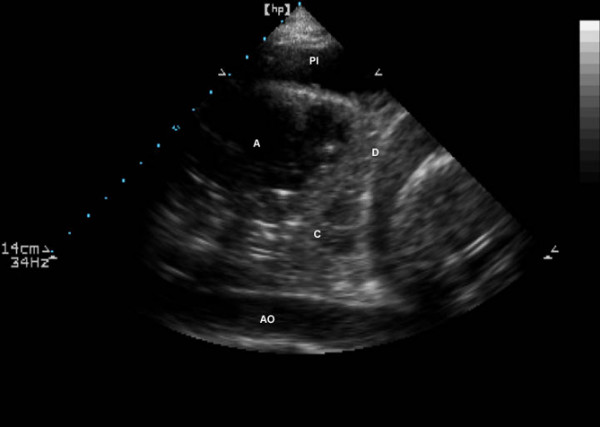
Cephalocaudal view of consolidated left lower lobe with a peripheral abscess. The abscess (A) appears as rounded hypoechoic lesions inside a lung consolidation (C). Ao, descending aorta; D, diaphragm; Pl, pleural effusion.
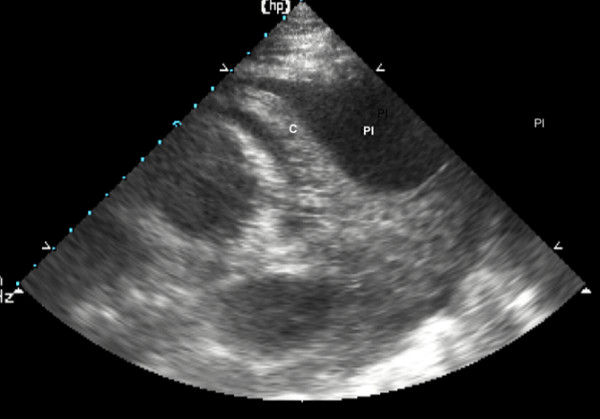
Consolidated lung 'floating' in a massive pleural effusion. The pleural effusion (Pl) is abundant enough to be compressive and the lung (C) is seen consolidated and floating in the pleural effusion.
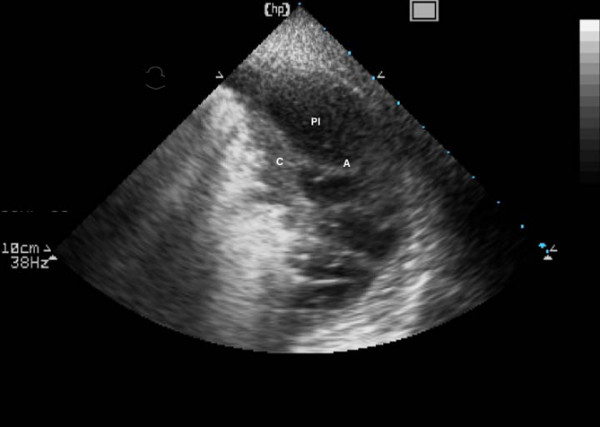
Consolidated lung and adjacent pleural effusion with pleural adherences. The pleural effusion (Pl) is abundant and the lung is seen consolidated and floating (C) in the pleural effusion with pleural adherences (A).
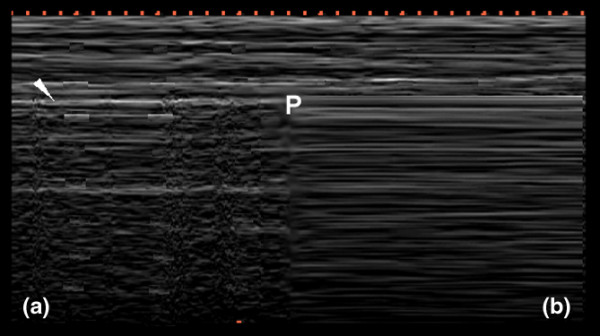
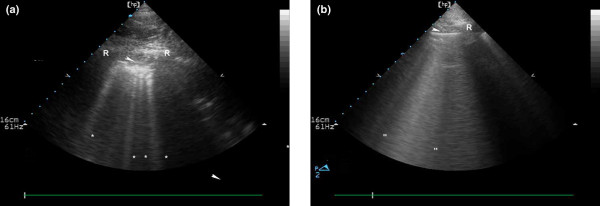
Time-motion mode lung ultrasound. (a) Normal lung and (b) pneumothorax patterns using time-motion mode lung ultrasound. In time motion mode, one must first locate the pleural line (white arrow) and, above it, the motionless parietal structures. Below the pleural line, lung sliding appears as a homogenous granular pattern (a). In the case of pneumothorax and absent lung sliding, horizontal lines only are visualised (b). In a patient examined in the supine position with partial pneumothorax, normal lung sliding and absence of lung sliding may coexist in lateral regions of the chest wall. In this boundary region, called the 'lung point' (P), lung sliding appears (granular pattern) and disappears (strictly horizontal lines) with inspiration when using the time-motion mode.
References
-
- Greenbaum DM, Marschall KE. The value of routine daily chest x-rays in intubated patients in the medical intensive care unit. Crit Care Med. 1982;10:29–30. - PubMed
-
- Bekemeyer WB, Crapo RO, Calhoon S, Cannon CY, Clayton PD. Efficacy of chest radiography in a respiratory intensive care unit. A prospective study. Chest. 1985;88:691–696. - PubMed
-
- Rouby JJ, Puybasset L, Cluzel P, Richecoeur J, Lu Q, Grenier P. Regional distribution of gas and tissue in acute respiratory distress syndrome. II. Physiological correlations and definition of an ARDS Severity Score. CT Scan ARDS Study Group. Intensive Care Med. 2000;26:1046–1056. doi: 10.1007/s001340051317. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
