

The heterogeneity of juvenile myositis
- PMID: 17317616
- PMCID: PMC1850932
- DOI: 10.1016/j.autrev.2006.08.009
The heterogeneity of juvenile myositis
Abstract
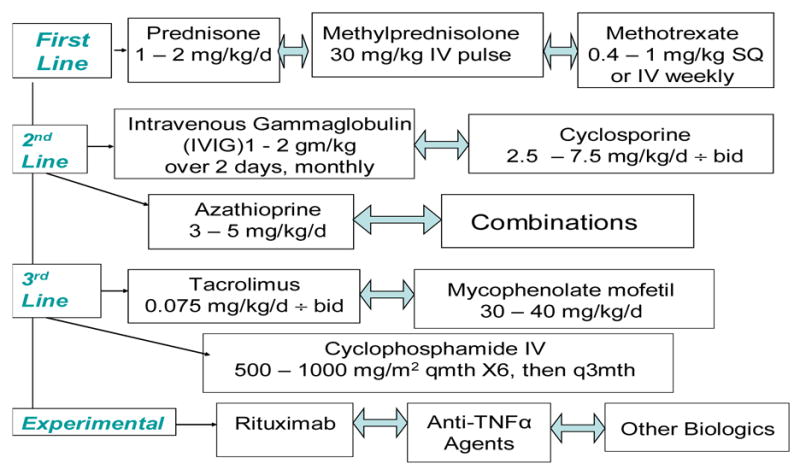
Juvenile myositis is a heterogeneous group of systemic autoimmune diseases, in which clinical and serologic subgroups result in subsets of patients with distinct clinical manifestations, disease courses, immunogenetic associations, responses to therapy, and prognoses. A newly identified autoantibody of unknown specificity, anti-p155, is myositis-associated and seen in up to 20-30% of juvenile and adult DM patients. HLA DRB1*0301 and its linked allele DQA1*0501 have been identified as the major immunogenetic risk factor for juvenile and adult DM in both European- and African-American patients, and DQA1*0301 is an additional risk factor in European-American patients. Several DQA1 alleles also are protective for juvenile DM. Environmental risk factors are poorly understood, but growing evidence suggests a role for infectious agents and ultraviolet radiation. The current therapy of juvenile DM consists of corticosteroids and other immunosuppressive agents, with the adjunctive treatment of cutaneous manifestations and rehabilitation. Therapeutic trials of biologic agents, including anti-TNFalpha and anti-CD20, may aid in developing promising new therapies for these disorders.
Figures
Similar articles
-
Immunogenetic risk and protective factors for the idiopathic inflammatory myopathies: distinct HLA-A, -B, -Cw, -DRB1, and -DQA1 allelic profiles distinguish European American patients with different myositis autoantibodies.Medicine (Baltimore). 2006 Mar;85(2):111-127. doi: 10.1097/01.md.0000217525.82287.eb. Medicine (Baltimore). 2006. PMID: 16609350
-
Immunogenetic risk and protective factors for juvenile dermatomyositis in Caucasians.Arthritis Rheum. 2006 Dec;54(12):3979-87. doi: 10.1002/art.22216. Arthritis Rheum. 2006. PMID: 17133612 Free PMC article.
-
HLA polymorphisms in African Americans with idiopathic inflammatory myopathy: allelic profiles distinguish patients with different clinical phenotypes and myositis autoantibodies.Arthritis Rheum. 2006 Nov;54(11):3670-81. doi: 10.1002/art.22205. Arthritis Rheum. 2006. PMID: 17075818
-
HLA-D region genes associated with autoantibody responses to histidyl-transfer RNA synthetase (Jo-1) and other translation-related factors in myositis.Arthritis Rheum. 1990 Aug;33(8):1240-8. doi: 10.1002/art.1780330826. Arthritis Rheum. 1990. PMID: 1975177 Review.
-
Developments in the classification and treatment of the juvenile idiopathic inflammatory myopathies.Rheum Dis Clin North Am. 2013 Nov;39(4):877-904. doi: 10.1016/j.rdc.2013.06.001. Epub 2013 Sep 19. Rheum Dis Clin North Am. 2013. PMID: 24182859 Free PMC article. Review.
Cited by
-
Juvenile dermatomyositis: the role of cytokine gene polymorphisms in conferring risk and protection.Curr Rheumatol Rep. 2009 Jul;11(3):164-6. doi: 10.1007/s11926-009-0033-1. Curr Rheumatol Rep. 2009. PMID: 19604459 No abstract available.
-
Biologic drugs in the treatment of juvenile dermatomyositis: a literature review.Clin Rheumatol. 2024 Feb;43(2):591-602. doi: 10.1007/s10067-023-06740-3. Epub 2023 Aug 16. Clin Rheumatol. 2024. PMID: 37582998 Review.
-
Biologic therapies for refractory juvenile dermatomyositis: five years of experience of the Childhood Arthritis and Rheumatology Research Alliance in North America.Pediatr Rheumatol Online J. 2017 Jun 13;15(1):50. doi: 10.1186/s12969-017-0174-0. Pediatr Rheumatol Online J. 2017. PMID: 28610606 Free PMC article.
-
A national registry for juvenile dermatomyositis and other paediatric idiopathic inflammatory myopathies: 10 years' experience; the Juvenile Dermatomyositis National (UK and Ireland) Cohort Biomarker Study and Repository for Idiopathic Inflammatory Myopathies.Rheumatology (Oxford). 2011 Jan;50(1):137-45. doi: 10.1093/rheumatology/keq261. Epub 2010 Sep 7. Rheumatology (Oxford). 2011. PMID: 20823094 Free PMC article.
-
The MHC locus and genetic susceptibility to autoimmune and infectious diseases.Genome Biol. 2017 Apr 27;18(1):76. doi: 10.1186/s13059-017-1207-1. Genome Biol. 2017. PMID: 28449694 Free PMC article. Review.
References
-
- Mendez EP, Lipton R, Ramsey-Goldman R, Roettcher P, Bowyer S, Dyer A, et al. US incidence of juvenile dermatomyositis, 1995–1998: results from the National Institute of Arthritis and Musculoskeletal and Skin Diseases Registry. Arthritis Rheum. 2003;49(3):300–305. - PubMed
-
- Pachman LM, Lipton R, Ramsey-Goldman R, Shamiyeh E, Abbott K, Mendez EP, et al. History of infection before the onset of juvenile dermatomyositis: results from the National Institute of Arthritis and Musculoskeletal and Skin Diseases Research Registry. Arthritis Rheum. 2005;53(2):166–172. - PubMed
-
- Rider LG, Miller FW. Classification and treatment of the juvenile idiopathic inflammatory myopathies. Rheum Dis Clin North Am. 1997;23:619–655. - PubMed
-
- Huber AM, Lang B, LeBlanc CM, Birdi N, Bolaria RK, Malleson P, et al. Medium- and long-term functional outcomes in a multicenter cohort of children with juvenile dermatomyositis. Arthritis Rheum. 2000;43(3):541–549. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
