

Seizure-promoting effect of blood-brain barrier disruption
- PMID: 17319915
- PMCID: PMC4135474
- DOI: 10.1111/j.1528-1167.2007.00988.x
Seizure-promoting effect of blood-brain barrier disruption
Abstract
Purpose: It is generally accepted that blood-brain barrier (BBB) failure occurs as a result of CNS diseases, including epilepsy. However, evidences also suggest that BBB failure may be an etiological factor contributing to the development of seizures.
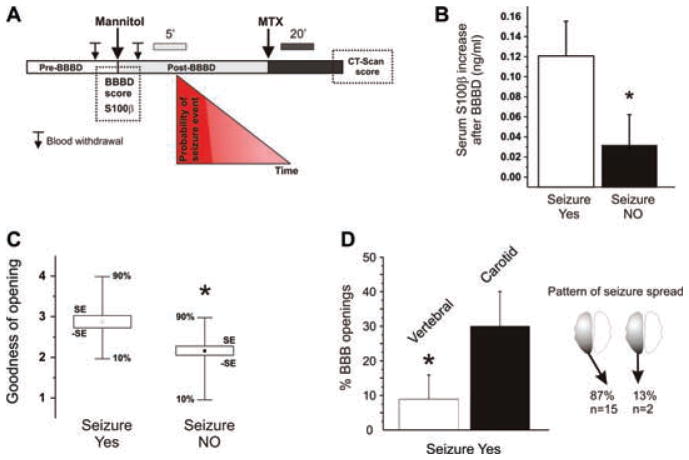
Methods: We monitored the onset of seizures in patients undergoing osmotic disruption of BBB (BBBD) followed by intraarterial chemotherapy (IAC) to treat primary brain lymphomas. Procedures were performed under barbiturate anesthesia. The effect of osmotic BBBD was also evaluated in naive pigs.
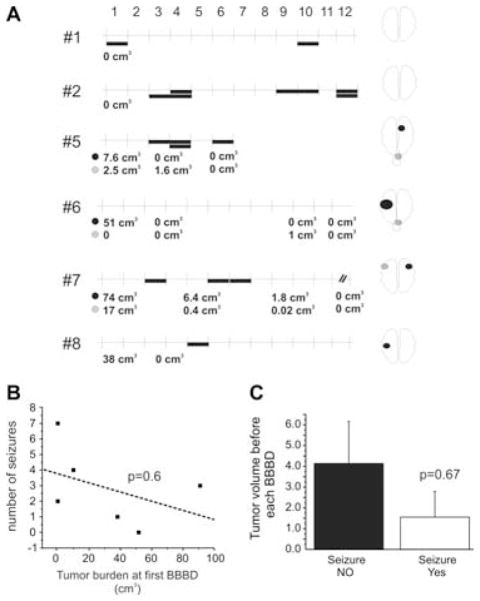
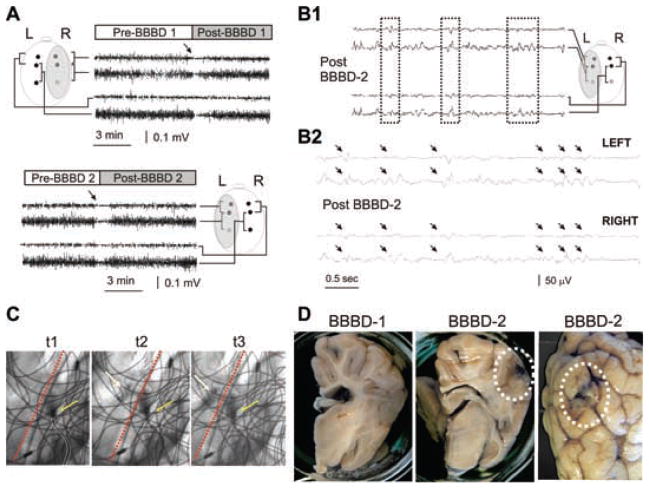
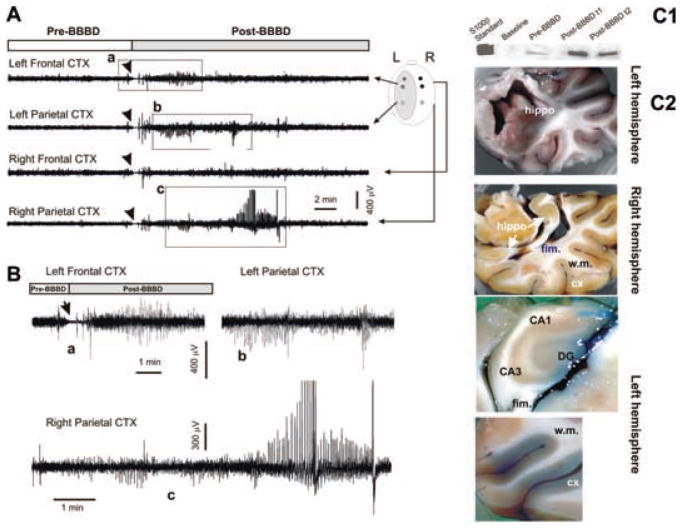
Results: Focal motor seizures occurred immediately after BBBD in 25% of procedures and originated contralateral to the hemisphere of BBBD. No seizures were observed when BBB was not breached and only IAC was administered. The only predictors of seizures were positive indices of BBBD, namely elevation of serum S100beta levels and computed tomography (CT) scans. In a porcine model of BBBD, identical procedures generated an identical result, and sudden behavioral and electrographic (EEG) seizures correlated with successful BBB disruption. The contribution of tumor or chemotherapy to acute seizures was therefore excluded.
Conclusion: This is the first study to correlate extent of acute BBB openings and development of seizures in humans and in a large animal model of BBB opening. Acute vascular failure is sufficient to cause seizures in the absence of CNS pathologies or chemotherapy.
Figures
References
-
- Alexander WS. Progressive fibrinoid degeneration of fibrillary astrocytes associated with mental retardation in a hydrocephalic infant. Brain. 1949;72:373–381. - PubMed
-
- Armstrong BK, Smith QR, Rapoport SI, Strohalm J, Kopacek J, Duncan R. Osmotic opening of the blood-brain barrier permeability to N-(2-hydroxypropyl) methacrylamide copolymers. Effects of polymer m.w., charge and hydrophobicity. Journal of Controlled Release. 1989;10:27–35.
-
- Clancy RR, Sharif U, Ichord R, Spray TL, Nicolson S, Tabbutt S, Wernovsky G, Gaynor JW. Electrographic neonatal seizures after infant heart surgery. Epilepsia. 2005;46:84–90. - PubMed
-
- Fazio V, Bhudia SK, Marchi N, Aumayr B, Janigro D. Peripheral detection of S100beta during cardiothoracic surgery: what are we really measuring? The Annals of Thoracic Surgery. 2004;78:46–52. - PubMed
-
- Fieschi C, Lenzi GL, Zanette E, Orzi F, Passero S. Effects on EEG of the osmotic opening of the blood-brain barrier in rats. Life Sciences. 1980;27:239–243. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
