

Lack of osteoradionecrosis of the mandible after intensity-modulated radiotherapy for head and neck cancer: likely contributions of both dental care and improved dose distributions
- PMID: 17321069
- PMCID: PMC2702207
- DOI: 10.1016/j.ijrobp.2006.11.059
Lack of osteoradionecrosis of the mandible after intensity-modulated radiotherapy for head and neck cancer: likely contributions of both dental care and improved dose distributions
Abstract
Purpose: To assess the prevalence and dosimetric and clinical predictors of mandibular osteoradionecrosis (ORN) in patients with head and neck cancer who underwent a pretherapy dental evaluation and prophylactic treatment according to a uniform policy and were treated with intensity-modulated radiotherapy (IMRT).
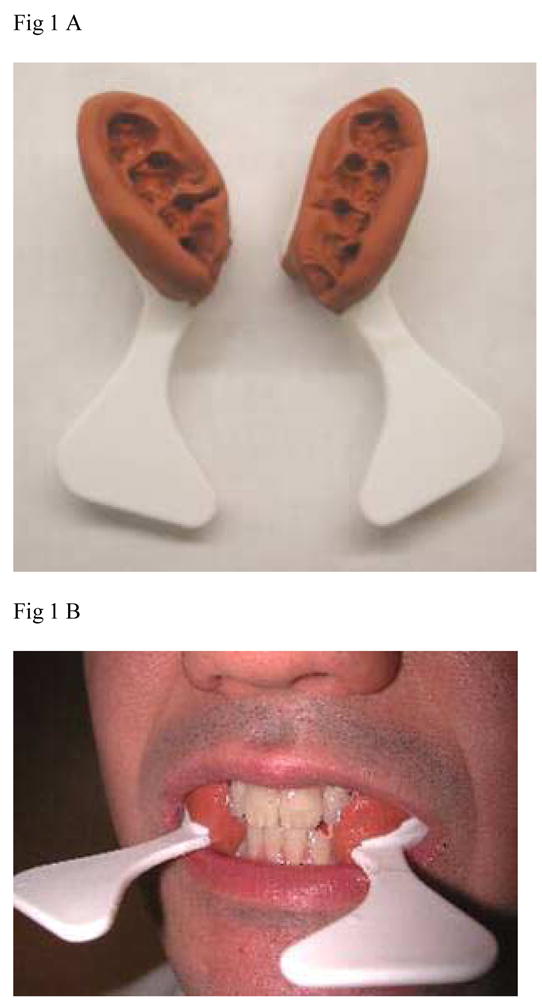
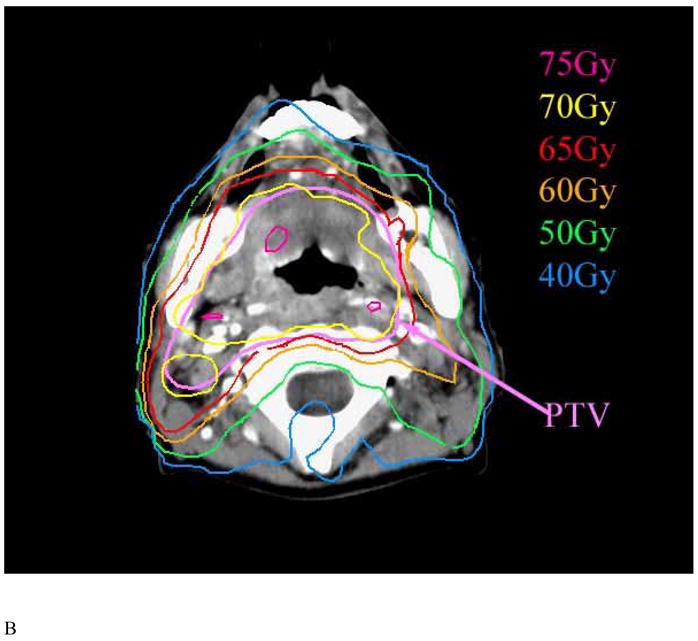
Methods and materials: Between 1996 and 2005, all patients with head-and-neck cancer treated with parotid gland-sparing IMRT in prospective studies underwent a dental examination and prophylactic treatment according to a uniform policy that included extractions of high-risk, periodontally involved, and nonrestorable teeth in parts of the mandible expected to receive high radiation doses, fluoride supplements, and the placement of guards aiming to reduce electron backscatter off metal teeth restorations. The IMRT plans included dose constraints for the maximal mandibular doses and reduced mean parotid gland and noninvolved oral cavity doses. A retrospective analysis of Grade 2 or worse (clinical) ORN was performed.
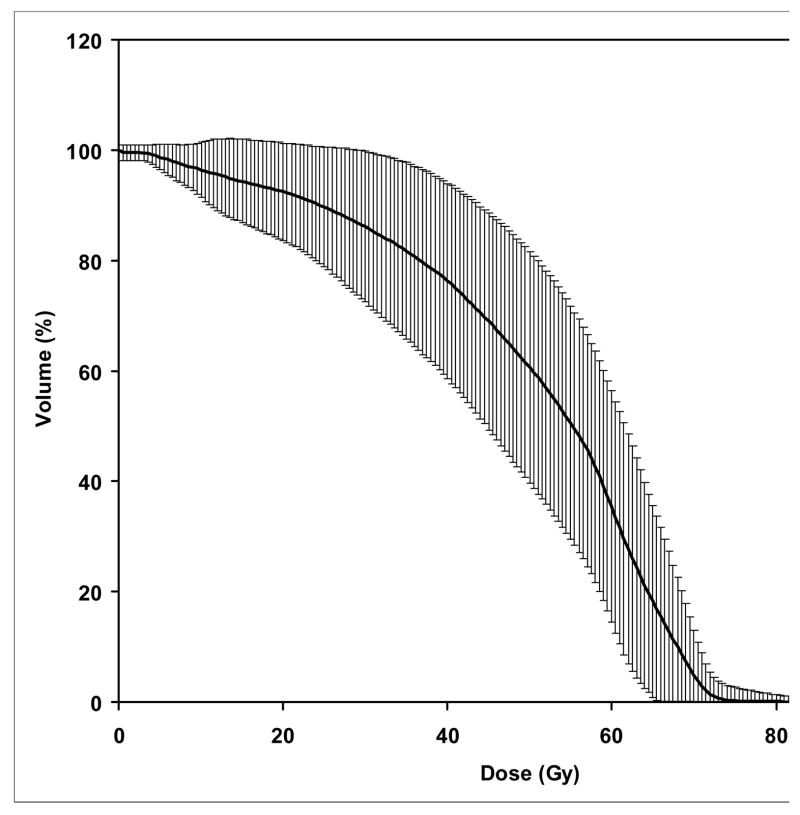
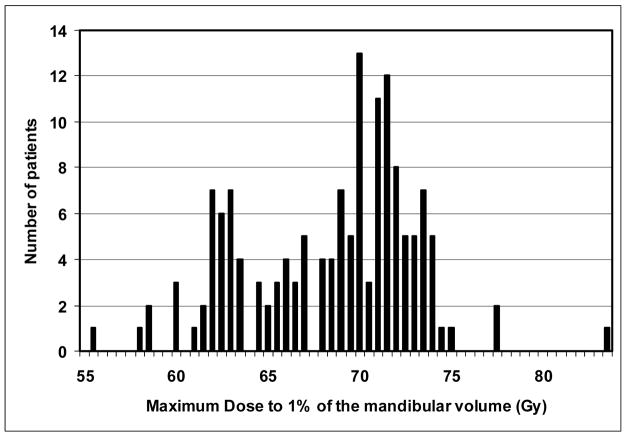
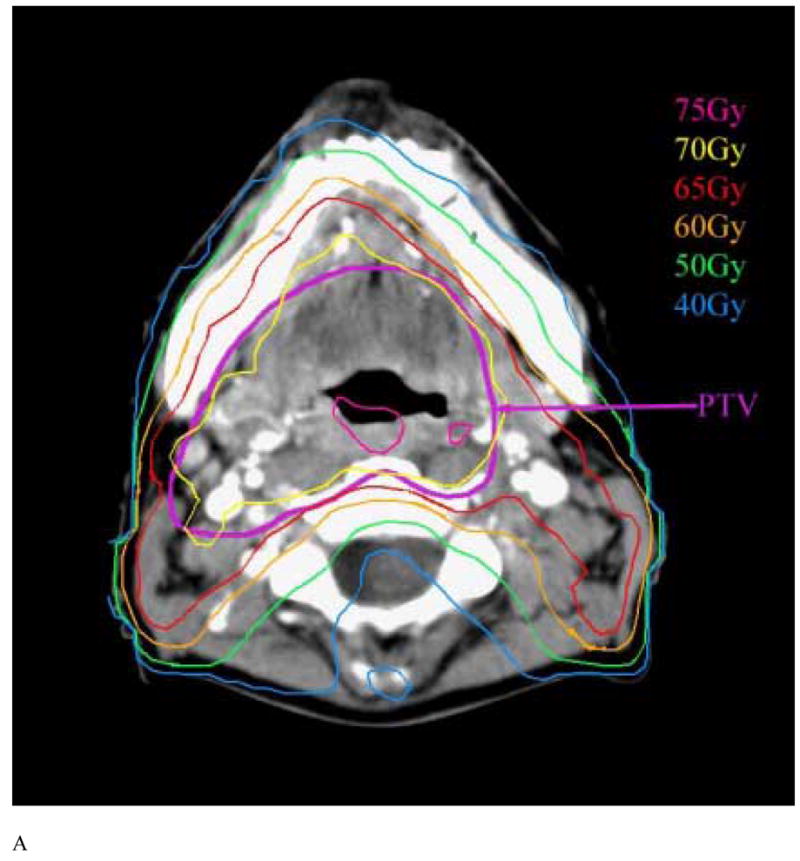
Results: A total of 176 patients had a minimal follow-up of 6 months. Of these, 31 (17%) had undergone teeth extractions before RT and 13 (7%) after RT. Of the 176 patients, 75% and 50% had received >or=65 Gy and >or=70 Gy to >or=1% of the mandibular volume, respectively. Falloff across the mandible characterized the dose distributions: the average gradient (in the axial plane containing the maximal mandibular dose) was 11 Gy (range, 1-27 Gy; median, 8 Gy). At a median follow-up of 34 months, no cases of ORN had developed (95% confidence interval, 0-2%).
Conclusion: The use of a strict prophylactic dental care policy and IMRT resulted in no case of clinical ORN. In addition to the dosimetric advantages offered by IMRT, meticulous dental prophylactic care is likely an essential factor in reducing ORN risk.
Conflict of interest statement
Figures
Comment in
-
In response to Dr. Merav A. Ben-David et al. ("Lack of osteoradionecrosis of the mandible after IMRT," Int J Radiat Oncol Biol Phys 2007:In Press).Int J Radiat Oncol Biol Phys. 2007 Aug 1;68(5):1583-4. doi: 10.1016/j.ijrobp.2007.04.030. Int J Radiat Oncol Biol Phys. 2007. PMID: 17674994 No abstract available.
References
-
- Wahl MJ. Osteoradionecrosis prevention myths. Int J Radiat Oncol Biol Phys. 2006;64(3):661–9. - PubMed
-
- Schwartz HC, Kagan AR. Osteoradionecrosis of the mandible: scientific basis for clinical staging. Am J Clin Oncol. 2002;25(2):168–71. - PubMed
-
- Mendenhall WM. Mandibular Osteoradionecrosis. J Clin Oncol. 2004;22(24):4867–4868. - PubMed
-
- Sciubba JS, Goldenberg D. Oral complications of radiotherapy. Lancet Oncol. 2006;7:175–83. - PubMed
-
- Eisbruch A, Foote RL, O’Sullivan B, Beitler JJ, Vikram B. Intensity-modulated radiation therapy for head and neck cancer: emphasis on the selection and delineation of the targets. Semin Radiat Oncol. 2002;12(3):238–49. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
