

Ectopic activity in the rat pulmonary vein can arise from simultaneous activation of alpha1- and beta1-adrenoceptors
- PMID: 17325650
- PMCID: PMC2013875
- DOI: 10.1038/sj.bjp.0707177
Ectopic activity in the rat pulmonary vein can arise from simultaneous activation of alpha1- and beta1-adrenoceptors
Abstract
Background and purpose: Atrial fibrillation (AF) is the most common electrical cardiac disorder in clinical practice. The major trigger for AF is focal ectopic activity of unknown origin in sleeves of cardiac muscle that extend into the pulmonary veins. We examined the role of noradrenaline in the genesis of ectopic activity in the pulmonary vein.
Experimental approach: Mechanical activity of strips of pulmonary vein isolated from male Wistar rats was recorded via an isometric tension meter. Twitch contractions of cardiac myocytes were evoked by electrical field stimulation in a tissue bath through which flowed Krebs-Heinseleit solution warmed to 36-37 degrees C and gassed with 95% O(2) 5% CO(2).
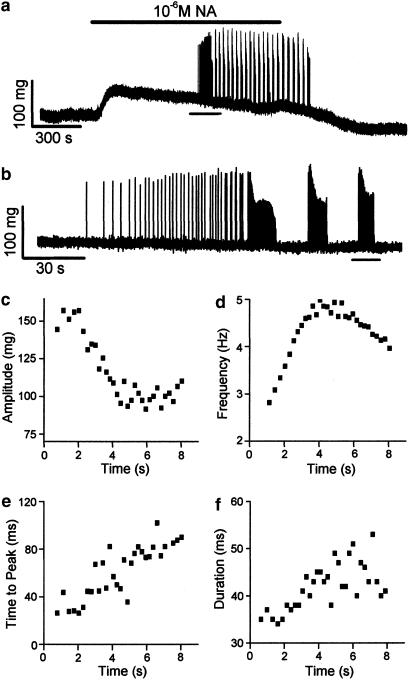
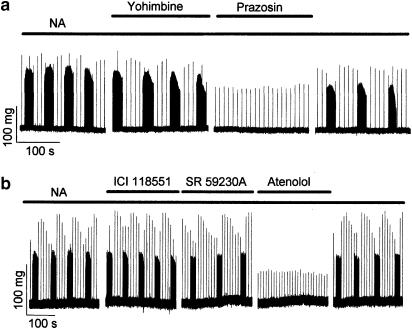
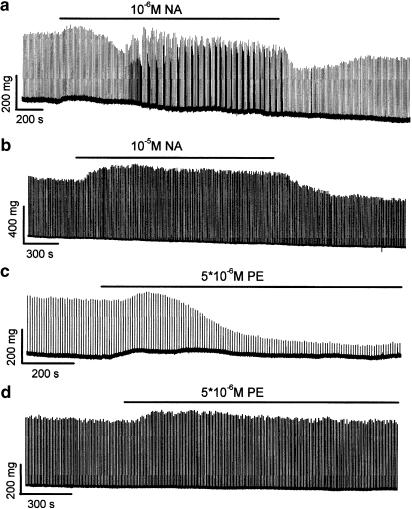
Key results: The superfusion of noradrenaline induced ectopic contractions in 71 of 76 different isolated pulmonary veins. Ectopic contractions in the pulmonary vein were not associated with electrically evoked twitch contractions. The effect of noradrenaline on the pulmonary vein could be replicated by the simultaneous, but not separate, application of the alpha adrenoceptor agonist phenylephrine and the beta adrenoceptor agonist isoprenaline. The use of selective agonists and antagonists for adrenoceptor subtypes showed that ectopic activity in the pulmonary vein arose from the simultaneous stimulation of alpha(1) and beta(1) adrenoceptors. The application of noradrenaline to isolated strips of left atrium did not induce ectopic contractions (n=10). conclusions: These findings suggest an origin for ectopic activity in the pulmonary vein that requires activation of both alpha and beta adrenoceptors. They also open new perspectives towards our understanding of the triggering of AF.
Figures



Similar articles
-
Testosterone protects rat hearts against ischaemic insults by enhancing the effects of alpha(1)-adrenoceptor stimulation.Br J Pharmacol. 2008 Feb;153(4):693-709. doi: 10.1038/sj.bjp.0707624. Epub 2007 Dec 24. Br J Pharmacol. 2008. PMID: 18157169 Free PMC article.
-
Arrhythmogenic coupling between the Na+ -Ca2+ exchanger and inositol 1,4,5-triphosphate receptor in rat pulmonary vein cardiomyocytes.J Mol Cell Cardiol. 2012 May;52(5):988-97. doi: 10.1016/j.yjmcc.2012.01.007. Epub 2012 Jan 20. J Mol Cell Cardiol. 2012. PMID: 22285480
-
beta-Adrenoceptors potentiate alpha1-adrenoceptor-mediated inotropic response in rat left atria.Acta Pharmacol Sin. 2004 Jan;25(1):29-34. Acta Pharmacol Sin. 2004. PMID: 14704119
-
Automatic Activity Arising in Cardiac Muscle Sleeves of the Pulmonary Vein.Biomolecules. 2021 Dec 24;12(1):23. doi: 10.3390/biom12010023. Biomolecules. 2021. PMID: 35053171 Free PMC article. Review.
-
Electrophysiological and pharmacological properties of the pulmonary vein myocardium.Biol Pharm Bull. 2013;36(1):2-7. doi: 10.1248/bpb.b212020. Biol Pharm Bull. 2013. PMID: 23302630 Review.
Cited by
-
Preferential Expression of Ca2+-Stimulable Adenylyl Cyclase III in the Supraventricular Area, including Arrhythmogenic Pulmonary Vein of the Rat Heart.Biomolecules. 2022 May 20;12(5):724. doi: 10.3390/biom12050724. Biomolecules. 2022. PMID: 35625651 Free PMC article.
-
Cardiovascular agents affect the tone of pulmonary arteries and veins in precision-cut lung slices.PLoS One. 2011;6(12):e29698. doi: 10.1371/journal.pone.0029698. Epub 2011 Dec 27. PLoS One. 2011. PMID: 22216346 Free PMC article.
-
Mechanisms Underlying Spontaneous Action Potential Generation Induced by Catecholamine in Pulmonary Vein Cardiomyocytes: A Simulation Study.Int J Mol Sci. 2019 Jun 14;20(12):2913. doi: 10.3390/ijms20122913. Int J Mol Sci. 2019. PMID: 31207916 Free PMC article.
-
Comparative study of hyperpolarization-activated currents in pulmonary vein cardiomyocytes isolated from rat, guinea pig, and rabbit.J Physiol Sci. 2020 Feb 11;70(1):6. doi: 10.1186/s12576-020-00736-3. J Physiol Sci. 2020. PMID: 32046630 Free PMC article.
-
Automaticity of the Pulmonary Vein Myocardium and the Effect of Class I Antiarrhythmic Drugs.Int J Mol Sci. 2024 Nov 18;25(22):12367. doi: 10.3390/ijms252212367. Int J Mol Sci. 2024. PMID: 39596432 Free PMC article. Review.
References
-
- Anderson RH, Brown NA, Moorman AFM. Development and structures of the venous pole of the heart. Dev Dyn. 2006;235:2–9. - PubMed
-
- Anderson RH, Ho SY. “Specialised” conducting cells in the pulmonary vein. J Cardiovasc Electrophysiol. 2004;15:121. - PubMed
-
- Biel M, Schneider A, Wahl C. Cardiac HCN channels: structure, function, and modulation. Trends Cardiovasc Med. 2002;12:206–213. - PubMed
-
- Bosch RF, Nattel S. Cellular electrophysiology of atrial fibrillation. Cardiovasc Res. 2002;54:259–269. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
