

Chemotherapy in advanced biliary tract carcinoma: a pooled analysis of clinical trials
- PMID: 17325704
- PMCID: PMC2360111
- DOI: 10.1038/sj.bjc.6603648
Chemotherapy in advanced biliary tract carcinoma: a pooled analysis of clinical trials
Abstract
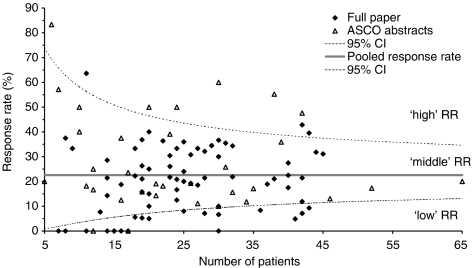
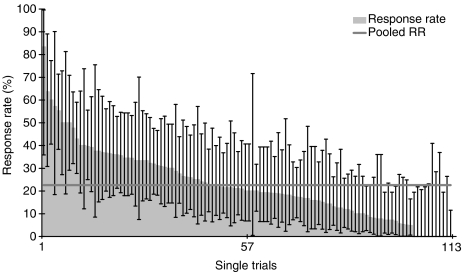
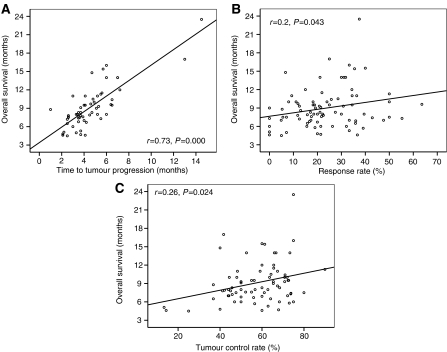
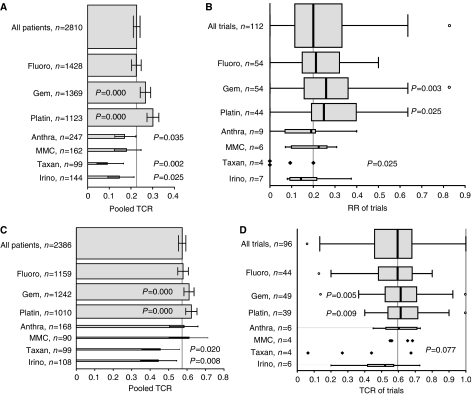
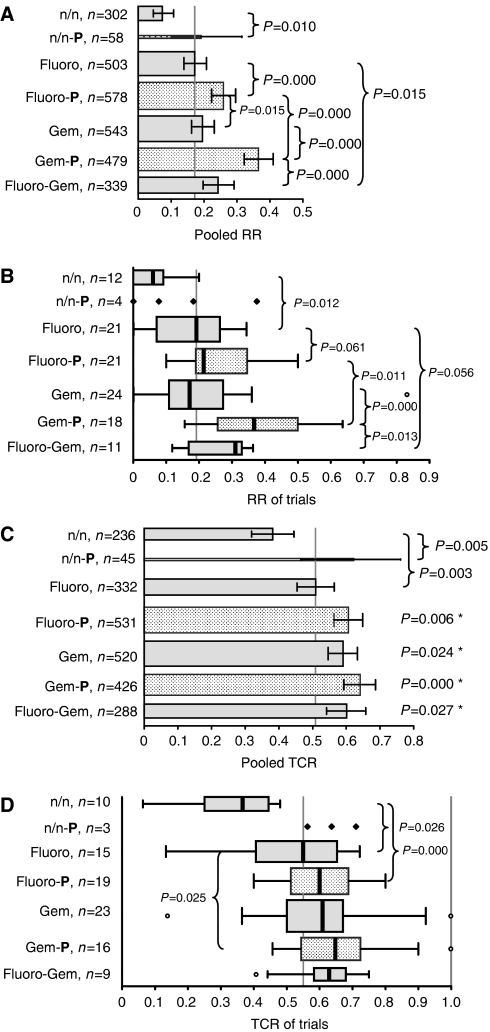
Owing to the lack of randomised controlled trials no standard of chemotherapy exists in the treatment of advanced biliary tract carcinoma. 5-fluorouracil or gemcitabine is recommended based on small and predominately phase II trials. The aim of this analysis was to analyse existing trials, even small and nonrandomised, and identify superior regimens. Chemotherapy trials published in English from 1985 to July 2006 were analysed as well as ASCO abstracts from 1999 to 2006. Response rate (RR=CR+PR), tumour control rate (TCR=CR+PR+SD), time to tumour progression (TTP), overall survival (OS), and toxicity were analysed. One hundred and four trials comprising 112 trial arms and 2810 patients, thereof 634 responders and 1368 patients with tumour control were analysed. Pooled RR and TCR were 22.6 and 57.3%, respectively. Significant correlations of RR and TCR with survival times were found. Subgroup analysis showed superior RRs for gallbladder carcinoma (GBC) compared with cholangiocarcinoma, but shorter OS for GBC. Furthermore, superior RRs and TCRs of gemcitabine and platinum containing regimens were found with highest RRs and TCRs in the combination subgroup. Based on published results of predominately phase II trials, gemcitabine combined with platinum compounds represents the provisional standard of chemotherapy in advanced biliary tract cancer, unless a new evidence-based standard has been defined.
Figures
References
-
- de Groen PC, Gores GJ, LaRusso NF, Gunderson LL, Nagorney DM (1999) Biliary tract cancers. N Engl J Med 341: 1368–1378 - PubMed
-
- Djulbegovic B, Frohlich A, Bennett CL (2005) Acting on imperfect evidence: how much regret are we ready to accept? J Clin Oncol 23: 6822–6825 - PubMed
-
- Ducreux M, Van Cutsem E, Van Laethem JL, Gress TM, Jeziorski K, Rougier P, Wagener T, Anak O, Baron B, Nordlinger B (2005) A randomised phase II trial of weekly high-dose 5-fluorouracil with and without folinic acid and cisplatin in patients with advanced biliary tract carcinoma: results of the 40955 EORTC trial. Eur J Cancer 41: 398–403 - PubMed
-
- Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD (2005) Cholangiocarcinoma. Lancet 366: 1303–1314 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
