

Whole body MR imaging in ankylosing spondylitis: a descriptive pilot study in patients with suspected early and active confirmed ankylosing spondylitis
- PMID: 17326845
- PMCID: PMC1810253
- DOI: 10.1186/1471-2474-8-20
Whole body MR imaging in ankylosing spondylitis: a descriptive pilot study in patients with suspected early and active confirmed ankylosing spondylitis
Abstract
Background: Ankylosing spondylitis is a chronic inflammatory rheumatic disorder which usually begins in early adulthood. The diagnosis is often delayed by many years. MR imaging has become the preferred imaging method for detection of early inflammation of the axial skeleton in ankylosing spondylitis. The goal of this study was to assess the frequency and distribution of abnormalities on whole body MR imaging in patients with suspected early ankylosing spondylitis and with active confirmed ankylosing spondylitis.
Methods: Ten patients with suspected early ankylosing spondylitis and ten patients with confirmed ankylosing spondylitis were enrolled. On an 18-channel MR system, coronal and sagittal T1 weighted and STIR sequences were acquired covering the entire spine, sacrum, anterior chest wall, shoulder girdle, and pelvis. The total examination time was 30 minutes.
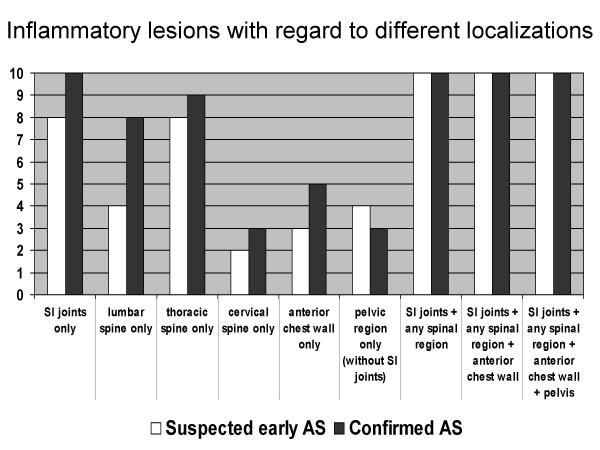
Results: In both groups inflammatory lesions of the lower thoracic spine were frequent (number of patients with suspected early/confirmed ankylosing spondylitis: 7/9). In confirmed ankylosing spondylitis the upper thoracic spine (3/6) and the lumbar spine (4/8) were more commonly involved. The inferior iliac quadrant of the sacroiliac joints was frequently altered in both groups (8/8). The superior iliac (2/5), inferior sacral (6/10) and superior sacral (3/6) quadrants were more frequently affected in confirmed ankylosing spondylitis. Abnormalities of the manubriosternal joint (2/4), the sternoclavicular joints (1/2) and hip joint effusion (4/3) were also seen.
Conclusion: In both suspected early ankylosing spondylitis and confirmed ankylosing spondylitis, whole body MR examinations frequently demonstrate inflammatory lesions outside the sacroiliac joints. These lesions are similarly distributed but occur less frequently in suspected early compared to confirmed ankylosing spondylitis. Due to the small sample size in this pilot study these results need to be confirmed in larger studies with this emerging technique.
Figures






References
-
- Boonen A, van der Heijde D, Landewé R, Guillemin F, Rutten-van Mölken M, Dougados M, Mielants H, de Vlam K, van der Tempel H, Boesen S, Spoorenberg A, Schouten H, van der Linden Sj. Direct costs of ankylosing spondylitis and its determinants: an analysis among three European countries. Ann Rheum Dis. 2003;62:732–740. doi: 10.1136/ard.62.8.732. - DOI - PMC - PubMed
-
- Boonen A, van der Heijde D, Landewé R, Spoorenberg A, Schouten H, Rutten-van Mölken M, Guillemin F, Dougados M, Mielants H, de Vlam K, van der Tempel H, van der Linden Sj. Work status and productivity costs due to ankylosing spondylitis: comparison of three European countries. Ann Rheum Dis. 2002;61:429–437. doi: 10.1136/ard.61.5.429. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
