

Using nurses to identify HAART eligible patients in the Republic of Mozambique: results of a time series analysis
- PMID: 17328804
- PMCID: PMC1817650
- DOI: 10.1186/1478-4491-5-7
Using nurses to identify HAART eligible patients in the Republic of Mozambique: results of a time series analysis
Abstract
Background: The most pressing challenge to achieving universal access to highly active anti-retroviral therapy (HAART) in sub-Saharan Africa is the shortage of trained personnel to handle the increased service requirements of rapid roll-out. Overcoming the human resource challenge requires developing innovative models of care provision that improve efficiency of service delivery and rationalize use of limited resources.
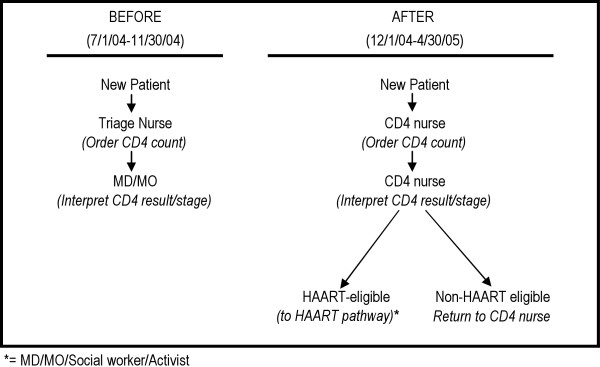
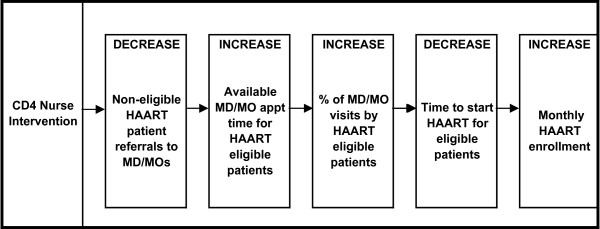
Methods: We conducted a time-series intervention trial in two HIV clinics in central Mozambique to discern whether expanding the role of basic-level nurses to stage HIV-positive patients using CD4 counts and WHO-defined criteria would lead to more rapid information on patient status (including identification of HAART eligible patients), increased efficiency in the use of higher-level clinical staff, and increased capacity to start HAART-eligible patients on treatment.
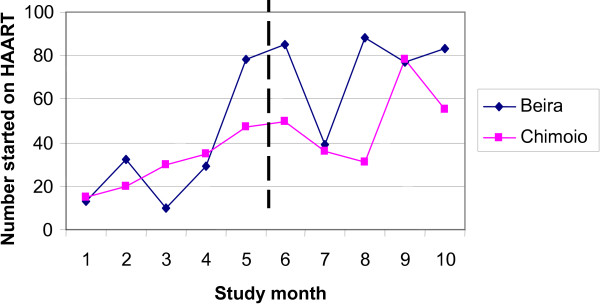
Results: Overall, 1,880 of the HAART-eligible patients were considered in the study of whom 48.5% started HAART, with a median time of 71 days from their initial blood draw. After adjusting for time, expanding the role of nurses to stage patients was associated with more rational use of higher-level clinical staff at one site (Beira OR 1.9, 95% CI 1.1-3.3; Chimoio OR 0.2, 95% CI 0.1-0.5). In multivariate analyses, the rate of starting HAART in patients with CD4 counts of less than 200/mm3 increased over time (HR = 1.07, 95% CI 1.02-1.13), as did the total number of new patients initiating HAART (beta = 7.3, 95% CI 1.3-13.3). However, the intervention was not independently associated with either of these outcomes in multivariate analyses (HR = 0.9, 95% CI 0.7-1.2) for starting HAART in patients with CD4 counts of less than 200/mm3; (beta = -5.2, p = 0.75) for the total number of new patients initiating HAART per month. No effect of the intervention was found in these outcomes when stratifying by site.
Conclusion: The CD4 nurse intervention, when implemented correctly, was associated with a more rational use of higher-level clinical providers, which may improve overall clinic flow and efficient use of the limited supply of human resources. However, this intervention did not lead to an increase in the number of patients starting HAART or a reduction in the time to HAART initiation. Study month appears to play an important role in all outcomes, suggesting that general improvements in clinic efficiency may have overshadowed the effect of the intervention. The lack of observed effect in these outcomes may be due to additional health systems bottlenecks that delay the initiation of treatment in HAART-eligible patients.
Figures
References
-
- World Health Organization (WHO) Progress on global access to HIV antiretroviral therapy. May 2006 http://www.who.int/hiv/progreport2006_summary_en.pdf
-
- World Health Organization (WHO) Progress in scaling up access to HIV treatment in low and middle-income countries, June 2006. UNAIDS. http://www.who.int/hiv/toronto2006/FS_Treatment_en.pdf
-
- Habte D, Dussault G, Dovlo D. Challenges confronting the health workforce in sub-Saharan Africa. The World Bank–World Hosp Health Serv. 2004;40:23–26. - PubMed
-
- Hosseinipour M, Kazembe P, Sanne I, van der Horst C. Challenges in delivering antiretroviral treatment in resource poor countries. AIDS. 2002;Suppl 4:177–187. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
