

doi: 10.1186/1471-2474-8-22.
Medial patellofemoral ligament reconstruction: a new technique
Affiliations
- PMID: 17328810
- PMCID: PMC1808455
- DOI: 10.1186/1471-2474-8-22
Item in Clipboard
Medial patellofemoral ligament reconstruction: a new technique
BMC Musculoskelet Disord.
.
Abstract
Background: Primary patellofemoral dislocations are common. In most patients, non-operative management produces satisfactory outcome. If the dislocation recurs after a trial of rehabilitation, operative intervention is considered, with the aim of restoring the soft tissue anatomy to normal. Ninety four percent of patients suffer a tear to the medial patellofemoral ligament (MPFL) following a patellar dislocation.
Results: We describe our transverse patella double tunnel technique to reconstruct the medial patellofemoral ligament using a free autologous gracilis or semitendinous graft.
Figures

Examination under anaesthesia revealing marked patella instability.
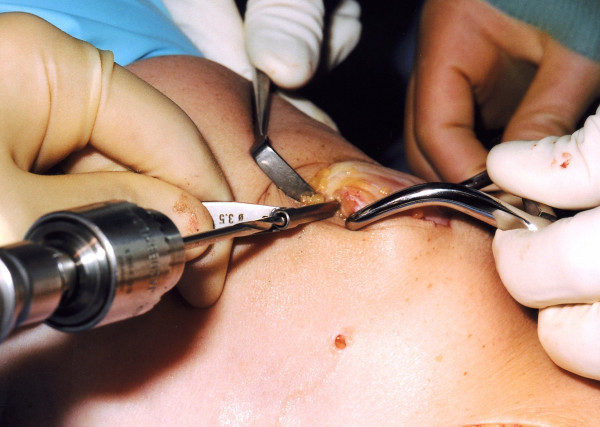
Following medial and lateral parapatellar incisions, the patella is stabilised using a large clamp on the right of the figure. Tunnels are produced by sequential drill holes in the superior half of the patella, 1 cm apart.

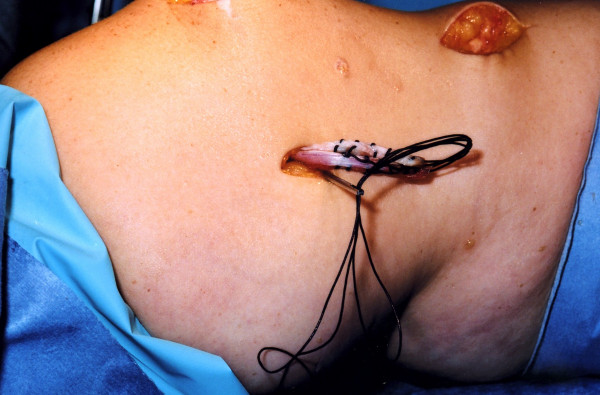
A Beath pin is used to pass a Vicryl loop through the patella tunnels.
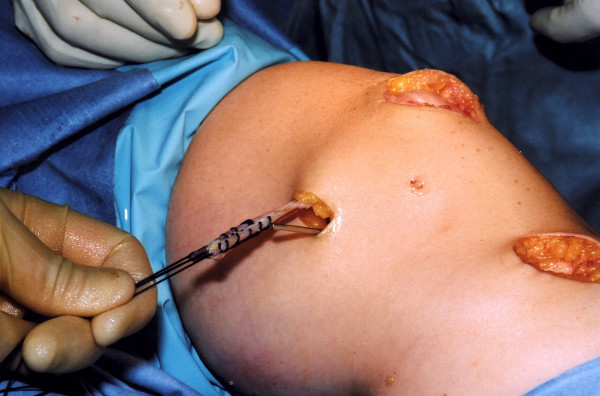
The graft is passed through the tunnels, laterally then medially.
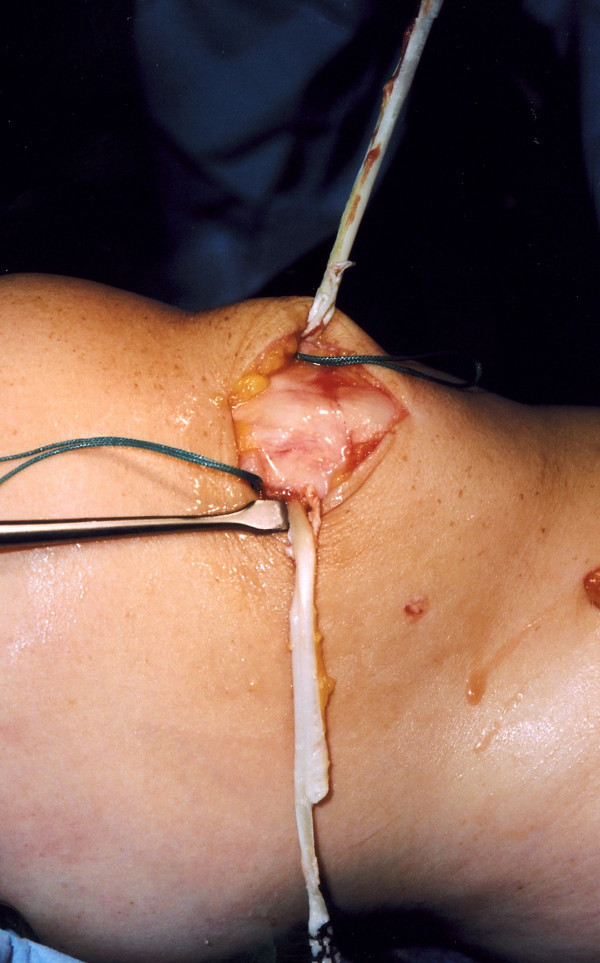
The medial epicondyle is exposed and the Beath pin is placed across the transepicondylar axis and a tunnel is drilled to accommodate and secure both ends of the graft. The graft is passed between the second and third layers of the knee.
The graft is pulled into the tunnel using Vicryl through the eye of the Beath pin.

After cycling the knee through a full range of movements to allow graft tension to settle, the graft is secured using an interference fit screw.

The improved stability of the patella is confirmed.
Similar articles
-
Comparison of 2 different techniques for anatomic reconstruction of the medial patellofemoral ligament: a prospective randomized study.Am J Sports Med. 2013 May;41(5):1013-21. doi: 10.1177/0363546513480468. Epub 2013 Mar 22. Am J Sports Med. 2013. PMID: 23524153 Clinical Trial.
-
The Anatomy of the Medial Patellofemoral Ligament.Orthopedics. 2017 Jul 1;40(4):e583-e588. doi: 10.3928/01477447-20170223-03. Epub 2017 Feb 28. Orthopedics. 2017. PMID: 28241086 Review.
-
Lateral patellofemoral ligament reconstruction.Arthroscopy. 2004 Nov;20(9):998-1002. doi: 10.1016/j.arthro.2004.07.005. Arthroscopy. 2004. PMID: 15525935
-
Medial patellofemoral ligament reconstruction: indications and technique.Sports Med Arthrosc Rev. 2012 Sep;20(3):162-70. doi: 10.1097/JSA.0b013e318264188b. Sports Med Arthrosc Rev. 2012. PMID: 22878657 Review.
-
Medial patellofemoral ligament reconstruction fixed with a cylindrical bone plug and a grafted semitendinosus tendon at the original femoral site for recurrent patellar dislocation.Am J Sports Med. 2011 Jan;39(1):140-5. doi: 10.1177/0363546510377436. Epub 2010 Oct 7. Am J Sports Med. 2011. PMID: 20929934
Cited by
-
Modern management of patellar instability.Int Orthop. 2012 Dec;36(12):2447-56. doi: 10.1007/s00264-012-1669-4. Epub 2012 Oct 7. Int Orthop. 2012. PMID: 23052278 Free PMC article. Review.
-
Medial Patellofemoral Ligament Reconstruction: An Uncommon Solution for a Common Problem.Int J Appl Basic Med Res. 2022 Apr-Jun;12(2):144-147. doi: 10.4103/ijabmr.ijabmr_445_21. Epub 2022 May 10. Int J Appl Basic Med Res. 2022. PMID: 35754665 Free PMC article.
-
[Patella dislocation].Unfallchirurg. 2011 Apr;114(4):345-58; quiz 359. doi: 10.1007/s00113-011-2012-z. Unfallchirurg. 2011. PMID: 21465418 German.
-
A computed tomography cadaveric study of the radiological anatomy of the patella: the size of the patella correlates with bone bridge between tunnels and R angles are introduced for safe tunnel drilling during MPFL reconstruction.J Exp Orthop. 2021 Apr 17;8(1):29. doi: 10.1186/s40634-021-00348-9. J Exp Orthop. 2021. PMID: 33864169 Free PMC article.
-
I.S.Mu.L.T. first-time patellar dislocation guidelines.Muscles Ligaments Tendons J. 2017 May 10;7(1):1-10. doi: 10.11138/mltj/2017.7.1.001. eCollection 2017 Jan-Mar. Muscles Ligaments Tendons J. 2017. PMID: 28717605 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
