

The acceptability of waiting times for elective general surgery and the appropriateness of prioritising patients
- PMID: 17328816
- PMCID: PMC1847814
- DOI: 10.1186/1472-6963-7-32
The acceptability of waiting times for elective general surgery and the appropriateness of prioritising patients
Abstract
Background: Problematic waiting lists in public health care threaten the equity and timeliness of care provision in several countries. This study assesses different stakeholders' views on the acceptability of waiting lists in health care, their preferences for priority care of patients, and their judgements on acceptable waiting times for surgical patients.
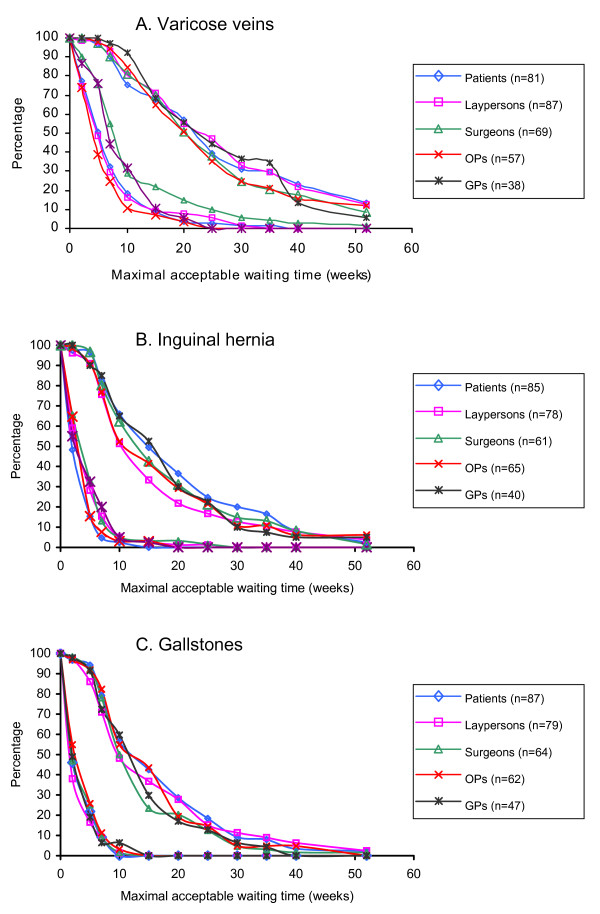
Methods: A questionnaire survey was conducted among 257 former patients (82 with varicose veins, 86 with inguinal hernia, and 89 with gallstones), 101 surgeons, 95 occupational physicians, and 65 GPs. Judgements on acceptable waiting times were assessed using vignettes of patients with varicose veins, inguinal hernia, and gallstones.
Results: Participants endorsed the prioritisation of patients based on clinical need, but not on ability to benefit. The groups had significantly different opinions (p < 0.05) on the use of non-clinical priority criteria and on the need for uniformity in the prioritisation process. Acceptable waiting times ranged between 2 and 25 weeks depending on the type of disorder (p < 0.001) and the severity of physical and psychosocial problems of patients (p < 0.001). Judgements were similar between the survey groups (p = 0.3) but responses varied considerably within each group depending on the individual's attitude towards waiting lists in health care (p < 0.001).
Conclusion: The explicit prioritisation of patients seems an accepted means for reducing the overall burden from waiting lists. The disagreement about appropriate prioritisation criteria and the need for uniformity, however, raises concern about equity when implementing prioritisation in daily practice. Single factor waiting time thresholds seem insufficient for securing timely care provision in the presence of long waiting lists as they do not account for the different consequences of waiting between patients.
Figures
Similar articles
-
Prioritising patients on surgical waiting lists: a conjoint analysis study on the priority judgements of patients, surgeons, occupational physicians, and general practitioners.Soc Sci Med. 2007 May;64(9):1863-75. doi: 10.1016/j.socscimed.2007.01.002. Epub 2007 Feb 26. Soc Sci Med. 2007. PMID: 17324491
-
Waiting for elective general surgery: impact on health related quality of life and psychosocial consequences.BMC Public Health. 2007 Jul 19;7:164. doi: 10.1186/1471-2458-7-164. BMC Public Health. 2007. PMID: 17640382 Free PMC article.
-
Waiting for elective surgery: effect on physical problems and postoperative recovery.ANZ J Surg. 2007 Oct;77(10):892-8. doi: 10.1111/j.1445-2197.2007.04268.x. ANZ J Surg. 2007. PMID: 17803558
-
Waiting for elective general surgery: physical, psychological and social consequences.ANZ J Surg. 2004 May;74(5):361-7. doi: 10.1111/j.1445-1433.2004.02998.x. ANZ J Surg. 2004. PMID: 15144258 Review.
-
[Waiting list guarantee between medicine and bureaucracy].Tidsskr Nor Laegeforen. 1998 Oct 20;118(25):3921-6. Tidsskr Nor Laegeforen. 1998. PMID: 9830336 Review. Norwegian.
Cited by
-
Surgical waiting times and patient choice: how much delay do patients really want?Eur J Orthop Surg Traumatol. 2015 Jan;25(1):77-81. doi: 10.1007/s00590-014-1460-x. Epub 2014 Apr 23. Eur J Orthop Surg Traumatol. 2015. PMID: 24756179
-
First Step to Equity and Organization in Waiting Lines for Stone Surgery. Translation of Prioritization Scores.Int Braz J Urol. 2025 Jul-Aug;51(4):e20250039. doi: 10.1590/S1677-5538.IBJU.2025.0039. Int Braz J Urol. 2025. PMID: 40327519 Free PMC article.
-
A Delphi study to explore clinician and lived experience perspectives on setting priorities in eating disorder services.BMC Health Serv Res. 2022 Jun 17;22(1):788. doi: 10.1186/s12913-022-08170-4. BMC Health Serv Res. 2022. PMID: 35715780 Free PMC article.
-
A model of access combining triage with initial management reduced waiting time for community outpatient services: a stepped wedge cluster randomised controlled trial.BMC Med. 2018 Oct 19;16(1):182. doi: 10.1186/s12916-018-1170-z. BMC Med. 2018. PMID: 30336784 Free PMC article. Clinical Trial.
-
Complications While Waiting for IBD Surgery-Short Report.J Crohns Colitis. 2020 Feb 10;14(2):277-280. doi: 10.1093/ecco-jcc/jjz143. J Crohns Colitis. 2020. PMID: 31402385 Free PMC article.
References
-
- Health Policy and Economic Research Unit, British Medical Association . Waiting list prioritisation scoring systems: a discussion paper. London, British Medical Association; 1998.
-
- Department of Health The NHS plan. A plan for investment. A plan for reform. London. 2002.
MeSH terms
LinkOut - more resources
Full Text Sources
