

Cost effectiveness analysis of minimally invasive internal thoracic artery bypass versus percutaneous revascularisation for isolated lesions of the left anterior descending artery
- PMID: 17337457
- PMCID: PMC1831990
- DOI: 10.1136/bmj.39112.480023.BE
Cost effectiveness analysis of minimally invasive internal thoracic artery bypass versus percutaneous revascularisation for isolated lesions of the left anterior descending artery
Abstract
Objective: To compare the cost effectiveness of percutaneous transluminal coronary artery stenting with minimally invasive internal thoracic artery bypass for isolated lesions of the left anterior descending artery.
Design: Cost effectiveness analysis.
Data sources: Embase, Medline, Cochrane, Google Scholar, and Health Technology Assessment databases (1966-2005), and reference sources for utility values and economical variables.
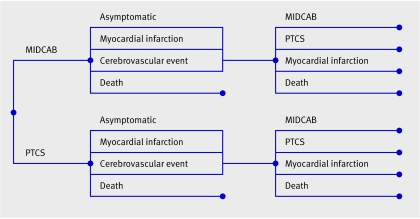
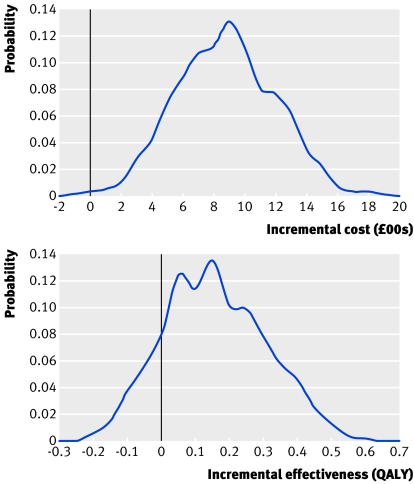
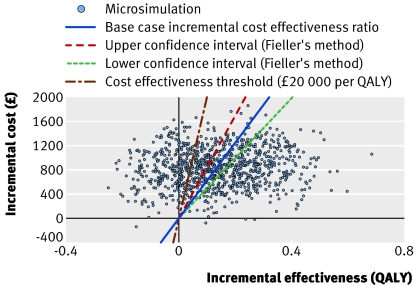
Methods: Decision analytical modelling and Markov simulation were used to model medium and long term costs, quality of life, and cost effectiveness after either intervention using data from referenced sources. Probabilistic sensitivity and alternative analyses were used to investigate the effect of uncertainty about the value of model variables and model structure.
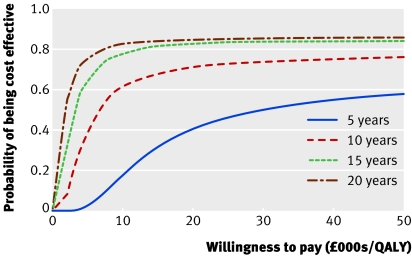
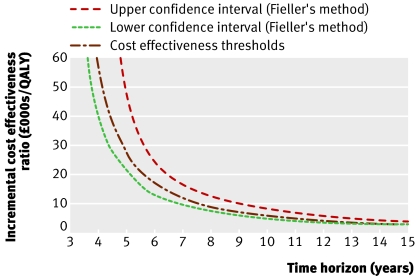
Results: Stenting was the dominant strategy in the first two years, being both more effective and less costly than bypass surgery. In the third year bypass surgery still remained more expensive but became marginally more effective. As the incremental cost effectiveness was 1,108,130.40 pounds sterling (1 682,146.00 euros; $2,179,194) per quality adjusted life year (QALY), the additional effectiveness could not be said to justify the additional cost at this stage. By five years, however, the incremental cost effectiveness ratio of 28,042.95 pounds sterling per QALY began to compare favourably with other interventions. At 10 years the additional effectiveness of 0.132 QALYs (range -0.166 to 0.430) probably justified the additional cost of 829.02 pounds sterling (range 205.56 pounds sterling to 1452.48 pounds sterling), with an incremental cost effectiveness of 6274.02 pounds sterling per QALY. Sensitivity and alternative analysis showed the results were sensitive to the time horizon and stent type.
Conclusions: Minimally invasive left internal thoracic artery bypass may be a more cost effective medium and long term alternative to percutaneous transluminal coronary artery stenting.
Conflict of interest statement
Figures
Comment in
-
Coronary revascularisation.BMJ. 2007 Mar 24;334(7594):593-4. doi: 10.1136/bmj.39154.552280.BE. BMJ. 2007. PMID: 17379861 Free PMC article.
-
To stent or not to stent?: A sterile debate.BMJ. 2007 Jul 21;335(7611):111. doi: 10.1136/bmj.39273.655694.BE. BMJ. 2007. PMID: 17641307 Free PMC article. No abstract available.
References
-
- Zimmerman FH, Cameron A, Fisher LD, Grace NG. Myocardial infarction in young adults: angiographic characterization, risk factors and prognosis (Coronary Artery Surgery Study Registry). J Am Coll Cardiol 1995;26:654-61. - PubMed
-
- Niinami H, Takeuchi Y, Ichikawa S, Suda Y. Partial median sternotomy as a minimal access for off-pump coronary artery bypass grafting: feasibility of the lower-end sternal splitting approach. Ann Thorac Surg 2001;72(3):S1041-5. - PubMed
-
- Casula R, Athanasiou T, Foale R. Recent advances in minimal-access cardiac surgery using robotic-enhanced surgical systems. Expert Rev Cardiovasc Ther 2004;2:589-600. - PubMed
-
- Aziz O, Rao C, Panesar SS, Jones C, Morris S, Darzi A, et al. Meta-analysis of minimally invasive internal thoracic artery bypass versus percutaneous revascularisation for isolated lesions of the left anterior descending artery. BMJ 2007;doi=10.1136/bmj.39106.476215.BE. - PMC - PubMed
-
- Gray DT, Veenstra DL. Comparative economic analyses of minimally invasive direct coronary artery bypass surgery. J Thorac Cardiovasc Surg 2003;125(3):618-24. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical