

Cost effectiveness of clinically appropriate decisions on alternative treatments for angina pectoris: prospective observational study
- PMID: 17339236
- PMCID: PMC1832000
- DOI: 10.1136/bmj.39129.442164.55
Cost effectiveness of clinically appropriate decisions on alternative treatments for angina pectoris: prospective observational study
Abstract
Objective: To assess whether revascularisation that is considered to be clinically appropriate is also cost effective.
Design: Prospective observational study comparing cost effectiveness of coronary artery bypass grafting, percutaneous coronary intervention, or medical management within groups of patients rated as appropriate for revascularisation.
Setting: Three tertiary care centres in London.
Participants: Consecutive, unselected patients rated as clinically appropriate (using a nine member Delphi panel) to receive coronary artery bypass grafting only (n=815); percutaneous coronary intervention only (n=385); or both revascularisation procedures (n=520).
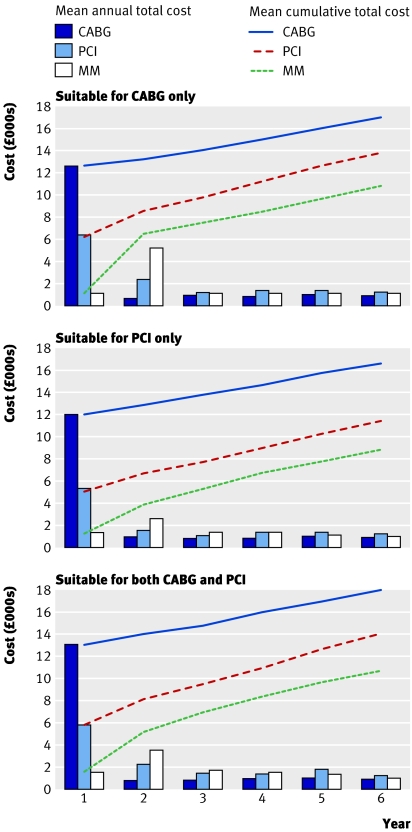
Main outcome measure: Cost per quality adjusted life year gained over six year follow-up, calculated with a National Health Service cost perspective and discounted at 3.5%/year.
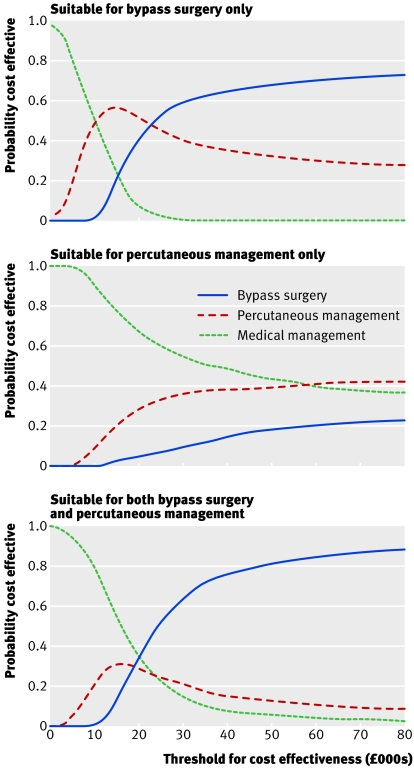
Results: Coronary artery bypass grafting cost 22,000 pounds sterling (33,000 euros; $43,000) per quality adjusted life year gained compared with percutaneous coronary intervention among patients appropriate for coronary artery bypass grafting only (59% probability of being cost effective at a cost effectiveness threshold of 30,000 pounds sterling per quality adjusted life year) and 19,000 pounds sterling per quality adjusted life year gained compared with medical management among those appropriate for both types of revascularisation (probability of being cost effective 63%). In none of the three appropriateness groups was percutaneous coronary intervention cost effective at a threshold of 30,000 pounds sterling per quality adjusted life year. Among patients rated appropriate for percutaneous coronary intervention only, the cost per quality adjusted life year gained for percutaneous coronary intervention compared with medical management was 47,000, pounds sterling exceeding usual cost effectiveness thresholds; in these patients, medical management was most likely to be cost effective (probability 54%).
Conclusions: Among patients judged clinically appropriate for coronary revascularisation, coronary artery bypass grafting seemed cost effective but percutaneous coronary intervention did not. Cost effectiveness analysis based on observational data suggests that the clinical benefit of percutaneous coronary intervention may not be sufficient to justify its cost.
Conflict of interest statement
Figures
Comment in
-
Coronary revascularisation.BMJ. 2007 Mar 24;334(7594):593-4. doi: 10.1136/bmj.39154.552280.BE. BMJ. 2007. PMID: 17379861 Free PMC article.
-
Case presented does not wash.BMJ. 2007 Apr 21;334(7598):813-4. doi: 10.1136/bmj.39185.447315.3A. BMJ. 2007. PMID: 17446579 Free PMC article. No abstract available.
-
To stent or not to stent?: A sterile debate.BMJ. 2007 Jul 21;335(7611):111. doi: 10.1136/bmj.39273.655694.BE. BMJ. 2007. PMID: 17641307 Free PMC article. No abstract available.
References
-
- Togni M, Balmer F, Pfiffner D, Maier W, Zeiher AM, Meier B, et al. Percutaneous coronary interventions in Europe 1992-2001. Eur Heart J 2004;25:1208-13. - PubMed
-
- Hueb W, Soares PR, Gersh BJ, César LAM, Luz PL, Puig LB, et al. The medicine, angioplasty, or surgery study (MASS-II): a randomized, controlled clinical trial of three therapeutic strategies for multivessel coronary artery disease. J Am Coll Cardiol 2004;43:1743-51. - PubMed
-
- Sculpher MJ, Smith DH, Clayton T, Henderson R, Buxton MJ, Pocock SJ, et al. Coronary angioplasty versus medical therapy for angina. Eur Heart J 2002;23:1291-300. - PubMed
-
- Claude J, Schindler C, Kuster GM, Schwenkglenks M, Szucs T, Buser P, et al. Cost-effectiveness of invasive versus medical management of elderly patients with chronic symptomatic coronary artery disease: findings of the randomized trial of invasive versus medical therapy in elderly patients with chronic angina (TIME). Eur Heart J 2004;25:2195-203. - PubMed
-
- Brook RH, Chassin MR, Fink A, Solomon DH, Kosecoff J, Park RE. A method for the detailed assessment of the appropriateness of medical technologies. Int J Technol Assess Health Care 1986;2:53-63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical