

Perfidious gallbladders - a diagnostic dilemma with xanthogranulomatous cholecystitis
- PMID: 17346415
- PMCID: PMC1964568
- DOI: 10.1308/003588407X155833
Perfidious gallbladders - a diagnostic dilemma with xanthogranulomatous cholecystitis
Abstract
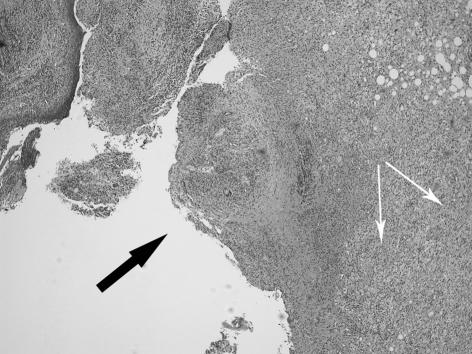
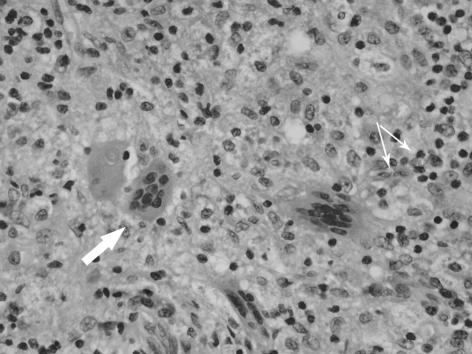
Introduction: Xanthogranulomatous cholecystitis (XGC) is an uncommon variant of chronic cholecystitis characterised by marked thickening of the gallbladder wall and dense local adhesions. Pre-operative and intra-operative diagnosis is difficult and it often mimics a gallbladder carcinoma (GBC). Laparoscopic cholecystectomy (LC) is frequently unsuccessful with a high conversion rate. A series of patients with this condition led us to review our experience with XGC and to try to develop a care pathway for its management.
Patients and methods: A retrospective review of the medical records of 1296 consecutive patients who had undergone cholecystectomy between January 2000 and April 2005 at our hospital was performed. Twenty-nine cases of XGC were identified among these cholecystectomies. The clinical, radiological and operative details of these patients have been analysed.
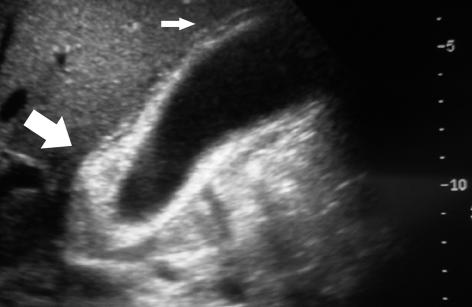
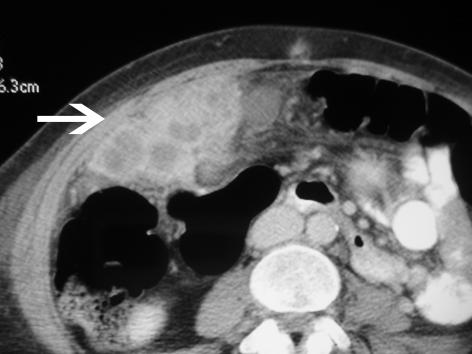
Results: The incidence of XGC was 2.2% in our study. The mean age at presentation was 60.3 years with a female:male ratio of 1.4:1. Twenty-three patients (79%) required an emergency surgical admission at first presentation. In three patients, a GBC was suspected both radiologically and at operation (10.3%), but was later disproved on histology. Seventeen patients (59%) had obstructive jaundice at first presentation and required an endoscopic retrograde cholangiopancreatography (ERCP) before LC. Of these, five had common bile duct stones. Abdominal ultrasound scan showed marked thickening of the gallbladder wall in 16 cases (55%). LC was attempted in 24 patients, but required conversion to an open procedure in 11 patients (46% conversion rate). A total cholecystectomy was possible in 18 patients and a partial cholecystectomy was the choice in 11 (38%). The average operative time was 96 min. Three patients developed a postoperative bile leak, one of whom required ERCP and placement of a biliary stent. The average length of stay in the hospital was 6.3 days.
Conclusions: Severe xanthogranulomatous cholecystitis often mimics a gallbladder carcinoma. Currently, a correct pre-operative diagnosis is rarely made. With increased awareness and a high index of suspicion, radiological diagnosis is possible. Preoperative counselling of these patients should include possible intra-operative difficulties and the differential diagnosis of gallbladder cancer. Laparoscopic cholecystectomy is frequently unsuccessful and a partial cholecystectomy is often the procedure of choice.
Figures
References
-
- Goodman ZD, Ishak KG. Xanthogranulomatous cholecystitis. Am J Surg Pathol. 1981;5:653–9. - PubMed
-
- Duber C, Storkel S, Wagner PK, Muller J. Xanthogranulomatous cholecystitis mimicking carcinoma of the gallbladder: CT findings. J Comput Assist Tomogr. 1984;8:1195–8. - PubMed
-
- Fligiel S, Lewin KJ. Xanthogranulomatous cholecystitis: case report and review of the literature. Arch Pathol Lab Med. 1982;106:302–4. - PubMed
-
- Solanki RL, Arora HL, Gaur SK, Anand VK, Gupta R. Xanthogranulomatous cholecystitis (XGC): a clinicopathological study of 21 cases. Indian J Pathol Microbiol. 1989;32:256–60. - PubMed
-
- Guzman-Valdivia G. Xanthogranulomatous cholecystitis: 15 years' experience. World J Surg. 2004;28:254–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous