

Neonatal diabetes mellitus: a disease linked to multiple mechanisms
- PMID: 17349054
- PMCID: PMC1847805
- DOI: 10.1186/1750-1172-2-12
Neonatal diabetes mellitus: a disease linked to multiple mechanisms
Abstract
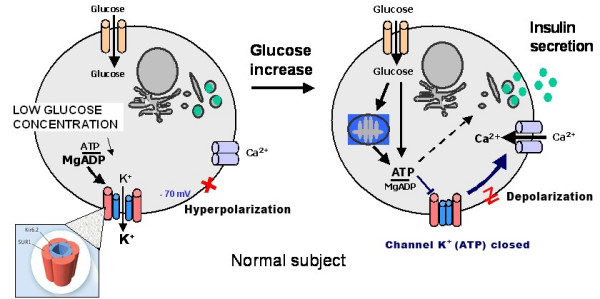
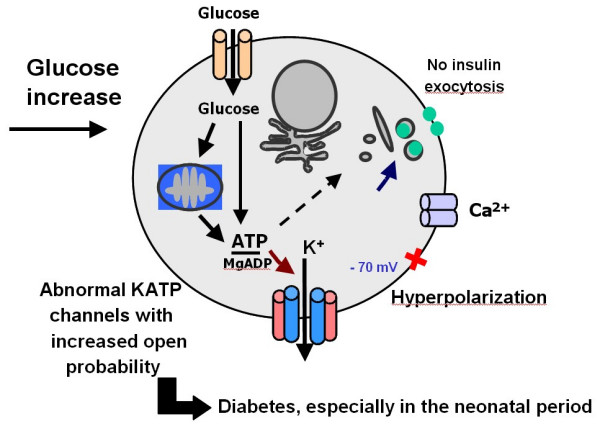
Transient (TNDM) and Permanent (PNDM) Neonatal Diabetes Mellitus are rare conditions occurring in 1:300,000-400,000 live births. TNDM infants develop diabetes in the first few weeks of life but go into remission in a few months, with possible relapse to a permanent diabetes state usually around adolescence or as adults. The pancreatic dysfunction in this condition may be maintained throughout life, with relapse initiated at times of metabolic stress such as puberty or pregnancy. In PNDM, insulin secretory failure occurs in the late fetal or early post-natal period and does not go into remission. Patients with TNDM are more likely to have intrauterine growth retardation and less likely to develop ketoacidosis than patients with PNDM. In TNDM, patients are younger at the diagnosis of diabetes and have lower initial insulin requirements. Considerable overlap occurs between the two groups, so that TNDM cannot be distinguished from PNDM based on clinical features. Very early onset diabetes mellitus seems to be unrelated to autoimmunity in most instances. A number of conditions are associated with PNDM, some of which have been elucidated at the molecular level. Among these, the very recently elucidated mutations in the KCNJ11 and ABCC8 genes, encoding the Kir6.2 and SUR1 subunit of the pancreatic KATP channel involved in regulation of insulin secretion, account for one third to half of the PNDM cases. Molecular analysis of chromosome 6 anomalies (found in more than 60% in TNDM), and the KCNJ11 and ABCC8 genes encoding Kir6.2 and SUR1, provides a tool to identify TNDM from PNDM in the neonatal period. This analysis also has potentially important therapeutic consequences leading to transfer some patients, those with mutations in KCNJ11 and ABCC8 genes, from insulin therapy to sulfonylureas. Recurrent diabetes is common in patients with "transient" neonatal diabetes mellitus and, consequently, prolonged follow-up is imperative. Realizing how difficult it is to take care of a child of this age with diabetes mellitus should prompt clinicians to transfer these children to specialized centers. Insulin therapy and high caloric intake are the basis of the treatment. Insulin pump may offer an interesting therapeutic tool in this age group in experienced hands.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
