

Osteoblastic and mixed spinal metastases: evaluation of the analgesic efficacy of percutaneous vertebroplasty
- PMID: 17353339
- PMCID: PMC7977851
Osteoblastic and mixed spinal metastases: evaluation of the analgesic efficacy of percutaneous vertebroplasty
Abstract
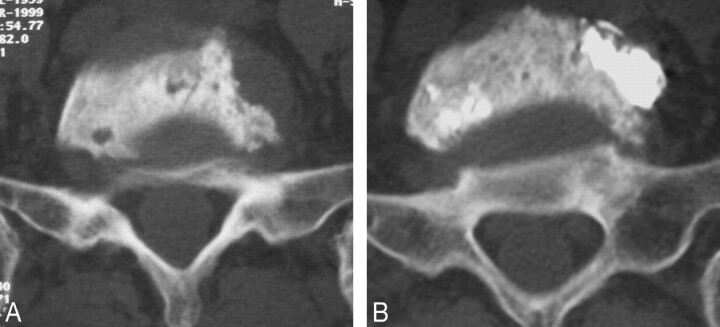
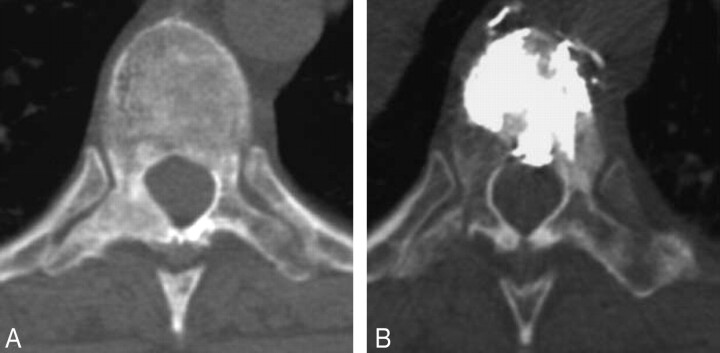
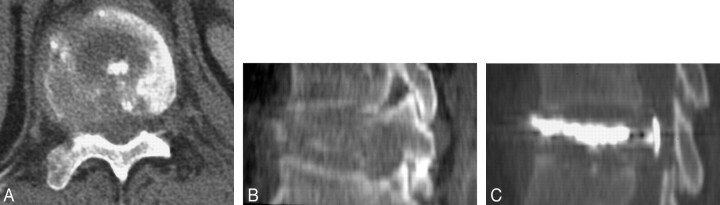
Purpose: To determine the analgesic efficacy of percutaneous vertebroplasty in treating osteoblastic and mixed spinal metastases.
Materials and methods: Fifty-two patients underwent 59 vertebroplasty procedures for 103 painful vertebral metastases, among which 53 were pure osteoblastic and 50 were mixed (blastic and lytic). Analgesic efficacy was classified as "excellent," "good," "fair," and "poor." The patients were followed up at 1 month, 6 months, 12 months, 2 years, and 5 years. The mean follow-up period was 17 months.
Results: The analgesic efficacy rate was 86% at 1 month and 92% at 6 months (among which 71% of patients had "excellent" results and 21% had with "good" results). In most cases, it was stable. It was correlated with vertebral filling quality (Fisher test, P = .0932 at 1 month follow-up) but neither with filling volume (Mann-Whitney test, P = .143 at 1 month) nor with the vertebral structure, pure blastic or mixed (Fisher test, P = .784 at 1 month). There were 5 filling failures (4.7%) whose occurrence was correlated with the pure blastic structure of the vertebra (Mann-Whitney test, P = .033). Local clinical complications were observed in 5 cases (8.5%): 1 transitory radiculalgia (1.7%), 2 durable radiculalgias (3.4%), 1 cauda equina syndrome (1.7%), and 1 hemothorax (1.7%). General clinical complications were 2 pulmonary embolisms (3.4%). No patients died. The occurrence of clinical complications was not correlated with the vertebral structure (Fisher test, P = .279).
Conclusion: Vertebroplasty for osteoblastic and mixed metastases allows, with a well-trained operator, a satisfactory anesthesia with acceptable clinical complication rates.
Figures
References
-
- Kallmes DF, Jensen ME. Percutaneous vertebroplasty. Radiology 2003;229:27–36 - PubMed
-
- Cotten A, Boutry N, Cortet B, et al. Percutaneous vertebroplasty: state of the art. Radiographics 1998;18:311–21 - PubMed
-
- Weill A, Chiras J, Simon JM, et al. Spinal metastases: indication for and results of percutaneous injection of acrylic chirurgical cement. Radiology 1996;199:241–47 - PubMed
-
- Barragan HM, Vallee JN, Lo D, et al. Percutaneous vertebroplasty for spinal metastases: complications. Radiology 2006;238:354–62 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical