

Safe liver resection following chemotherapy for colorectal metastases is a matter of timing
- PMID: 17353923
- PMCID: PMC2360122
- DOI: 10.1038/sj.bjc.6603670
Safe liver resection following chemotherapy for colorectal metastases is a matter of timing
Abstract
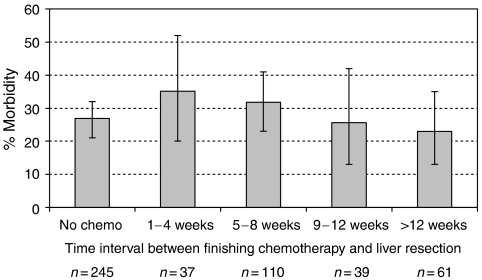
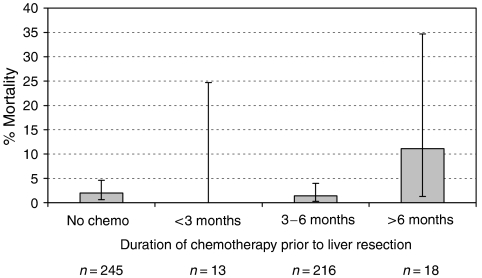
Neoadjuvant chemotherapy (NC) can improve the resectability of hepatic colorectal metastases (CRM). However, there is concern regarding its impact on operative risk. We reviewed 750 consecutive liver resections performed for CRM in a single unit (1996-2005) to evaluate whether NC affected morbidity and mortality. Redo hepatic resections or patients receiving adjuvant chemotherapy following primary resection were excluded. A total of 245 resections were performed in patients not requiring NC (control group) (mean age 63, 67% male) and 252 in patients who had NC (mean age 62, 67% male). The mean (s.d.) duration of surgery was less in the control group (241(64) vs 255(64)min, P=0.014) as was the mean blood loss (390(264) vs 449(424)ml, P=0.069). Postoperative mortality (2 vs 2%) and morbidity (27 vs 29%, P=0.34) was similar between groups. More NC patients developed septic (2.4%) or respiratory (10.3%) complications compared to controls (0 and 5.3%, P<0.03), with significantly more surgical complications if the interval between stopping NC and undergoing surgery was <or=4 weeks (11%), compared to 5-8 (5.5%) or 9-12 (2.6%) weeks (P=0.009). The data suggest that liver resection for CRM is safe following NC. Early hepatobiliary involvement in multidisciplinary cancer care may lead to avoidance of potential perioperative adverse events.
Figures

Similar articles
-
Chemotherapy for colorectal cancer prior to liver resection for colorectal cancer hepatic metastases does not adversely affect peri-operative outcomes.J Surg Oncol. 2007 Jan 1;95(1):22-7. doi: 10.1002/jso.20632. J Surg Oncol. 2007. PMID: 17066435
-
[HEMIHEPATECTOMY FOR RESECTABLE HEPATIC METASTASIS FROM COLORECTAL CANCER WITH POOR PROGNOSIS].Vopr Onkol. 2015;61(3):439-47. Vopr Onkol. 2015. PMID: 26242159 Clinical Trial. Russian.
-
Does neoadjuvant chemotherapy reveal disease precluding surgical treatment of initially resectable colorectal cancer liver metastases?J Surg Oncol. 2012 Jan;105(1):55-9. doi: 10.1002/jso.22044. Epub 2011 Aug 12. J Surg Oncol. 2012. PMID: 21842519 Clinical Trial.
-
[Colorectal cancer liver metastases -- neoadjuvant concepts for preoperative down-sizing].Zentralbl Chir. 2006 Apr;131(2):140-7. doi: 10.1055/s-2006-921538. Zentralbl Chir. 2006. PMID: 16612781 Review. German.
-
[Timing of resection in patients with colorectal carcinoma and synchronous liver metastases].Zentralbl Chir. 2009 Sep;134(5):425-9. doi: 10.1055/s-0029-1224612. Epub 2009 Sep 15. Zentralbl Chir. 2009. PMID: 19757342 Review. German.
Cited by
-
Post-hepatectomy liver failure in patients with colorectal liver metastases.Surg Today. 2015 Oct;45(10):1218-26. doi: 10.1007/s00595-015-1113-7. Epub 2015 Jan 29. Surg Today. 2015. PMID: 25628126 Review.
-
Chemotherapy-Associated Liver Injuries: Unmet Needs and New Insights for Surgical Oncologists.Ann Surg Oncol. 2021 Aug;28(8):4074-4079. doi: 10.1245/s10434-021-10069-z. Epub 2021 Apr 30. Ann Surg Oncol. 2021. PMID: 33929618 No abstract available.
-
The Relationship Between Postoperative Chemotherapy and Remnant Liver Regeneration and Outcomes After Hepatectomy for Colorectal Liver Metastasis.J Gastrointest Surg. 2019 Oct;23(10):1973-1983. doi: 10.1007/s11605-018-3952-1. Epub 2018 Sep 5. J Gastrointest Surg. 2019. PMID: 30187326
-
A meta-analysis of liver-first versus classical strategy for synchronous colorectal liver metastases.Int J Colorectal Dis. 2020 Mar;35(3):537-546. doi: 10.1007/s00384-020-03503-3. Epub 2020 Jan 18. Int J Colorectal Dis. 2020. PMID: 31955217
-
Diagnostic value/performance of radiological liver imaging during chemoterapy for gastrointestinal malignancy: a critical review.Acta Biomed. 2019 Apr 24;90(5-S):51-61. doi: 10.23750/abm.v90i5-S.8346. Acta Biomed. 2019. PMID: 31085973 Free PMC article. Review.
References
-
- Adam R, Avisar E, Ariche A, Giachetti S, Azoulay D, Castaing D, Kunstlinger F, Levi F, Bismuth F (2001) Five-year survival following hepatic resection after neoadjuvant therapy for nonresectable colorectal. Ann Surg Oncol 8: 347–353 - PubMed
-
- Allen PJ, Kemeny N, Jarnagin W, DeMatteo R, Blumgart L, Fong Y (2003) Importance of response to neoadjuvant chemotherapy in patients undergoing resection of synchronous colorectal liver metastases. J Gastrointest Surg 7: 109–115, discussion 116–117. - PubMed
-
- Basu S, Rees M, Tamijmaran A, Bygrave S, John TJ (2003) Influence of preoperative chemotherapy on recovery after hepatic resection for colorectal liver metastases. Br J Surg 90: 372
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
