

Nonventilatory treatments for acute lung injury and ARDS
- PMID: 17356114
- PMCID: PMC2789489
- DOI: 10.1378/chest.06-1743
Nonventilatory treatments for acute lung injury and ARDS
Abstract
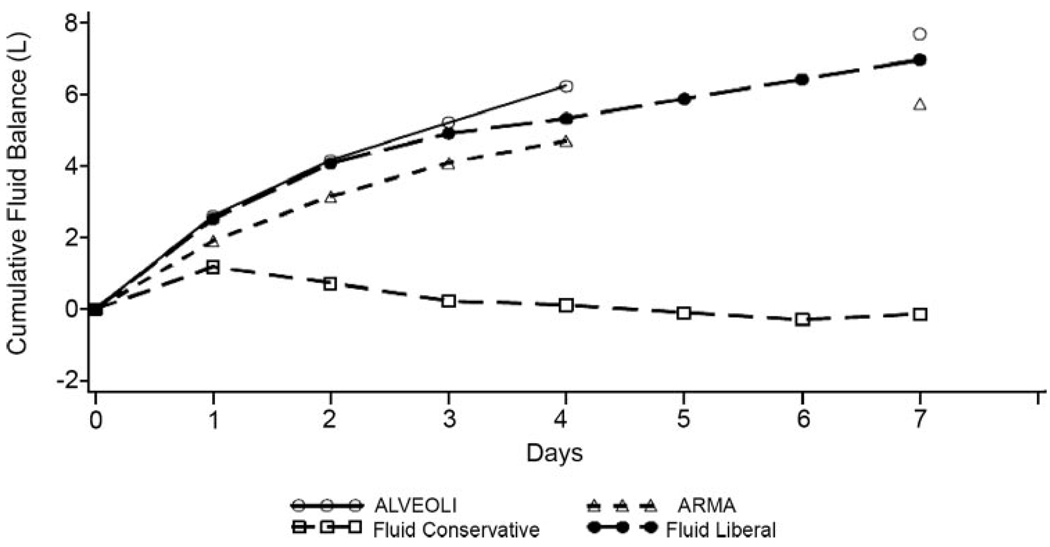
Over the past decade, advances in the ventilatory management of acute lung injury (ALI) and ARDS have improved outcomes; however, until recently the search for other therapies has been less fruitful. Recently, the Acute Respiratory Distress Syndrome Network Fluid and Catheter Treatment Trial reported that a conservative fluid management strategy, compared with a fluid liberal strategy, increased the mean (+/- SE) number of ventilator-free days in patients with ALI (14.6 +/- 0.5 vs 12.1 +/- 0.5 days, respectively; p < 0.001). In addition to this beneficial effect on outcomes, the study found that the conservative fluid strategy did not increase the incidence of renal failure or the development of shock. Other studies have demonstrated that albumin and furosemide therapy may be beneficial in hypoproteinemic patients with lung injury, though data on outcomes is still lacking. Although several pharmacologic therapies, such as corticosteroids, surfactant, and nitric oxide, have been demonstrated to be ineffective in improving outcomes, several promising new treatments are being investigated in ongoing or upcoming clinical trials. This article reviews these developments and other recent research on the optimal nonventilatory management of patients with ALI.
Conflict of interest statement
The authors have reported to the ACCP that no significant conflicts of interest exist with any companies/organizations whose products or services may be discussed in this article.
Figures
Comment in
-
Corticosteroids in ARDS: a counterpoint.Chest. 2007 Sep;132(3):1093-4; author reply 1094. doi: 10.1378/chest.07-0714. Chest. 2007. PMID: 17873207 No abstract available.
-
Nonventilatory treatments for ARDS?: future directions.Chest. 2008 Feb;133(2):586-7; author reply 587. doi: 10.1378/chest.07-2333. Chest. 2008. PMID: 18252932 No abstract available.
Similar articles
-
A randomized, controlled trial of furosemide with or without albumin in hypoproteinemic patients with acute lung injury.Crit Care Med. 2005 Aug;33(8):1681-7. doi: 10.1097/01.ccm.0000171539.47006.02. Crit Care Med. 2005. PMID: 16096441 Clinical Trial.
-
Recent developments in the management of acute respiratory distress syndrome in adults.Am J Health Syst Pharm. 2008 Jan 1;65(1):29-36. doi: 10.2146/ajhp060530. Am J Health Syst Pharm. 2008. PMID: 18159036 Review.
-
Comparison of two fluid-management strategies in acute lung injury.N Engl J Med. 2006 Jun 15;354(24):2564-75. doi: 10.1056/NEJMoa062200. Epub 2006 May 21. N Engl J Med. 2006. PMID: 16714767 Clinical Trial.
-
Less is more: improved outcomes in surgical patients with conservative fluid administration and central venous catheter monitoring.J Am Coll Surg. 2009 May;208(5):725-35; discussion 735-7. doi: 10.1016/j.jamcollsurg.2009.01.026. Epub 2009 Mar 31. J Am Coll Surg. 2009. PMID: 19476825 Clinical Trial.
-
Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med. 2008 Jan;36(1):296-327. doi: 10.1097/01.CCM.0000298158.12101.41. Crit Care Med. 2008. PMID: 18158437
Cited by
-
In vivo study of the effects of exogenous hydrogen sulfide on lung mitochondria in acute lung injury in rats.BMC Anesthesiol. 2014 Dec 15;14:117. doi: 10.1186/1471-2253-14-117. eCollection 2014. BMC Anesthesiol. 2014. PMID: 25550681 Free PMC article.
-
Evaluation of miRNAs Related with Nuclear Factor Kappa B Pathway in Lipopolysaccharide Induced Acute Respiratory Distress Syndrome.Int J Mol Cell Med. 2020 Spring;9(2):130-139. doi: 10.22088/IJMCM.BUMS.9.2.130. Epub 2020 Aug 10. Int J Mol Cell Med. 2020. PMID: 32934950 Free PMC article.
-
Early acute lung injury: criteria for identifying lung injury prior to the need for positive pressure ventilation*.Crit Care Med. 2013 Aug;41(8):1929-37. doi: 10.1097/CCM.0b013e31828a3d99. Crit Care Med. 2013. PMID: 23782966 Free PMC article.
-
Fat Embolism Syndrome - A Qualitative Review of its Incidence, Presentation, Pathogenesis and Management.Malays Orthop J. 2021 Mar;15(1):1-11. doi: 10.5704/MOJ.2103.001. Malays Orthop J. 2021. PMID: 33880141 Free PMC article. Review.
-
Mesenchymal stem cell: does it work in an experimental model with acute respiratory distress syndrome?Stem Cell Rev Rep. 2013 Feb;9(1):80-92. doi: 10.1007/s12015-012-9395-2. Stem Cell Rev Rep. 2013. PMID: 22810359 Free PMC article.
References
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med. 2004;351:327–336. - PubMed
-
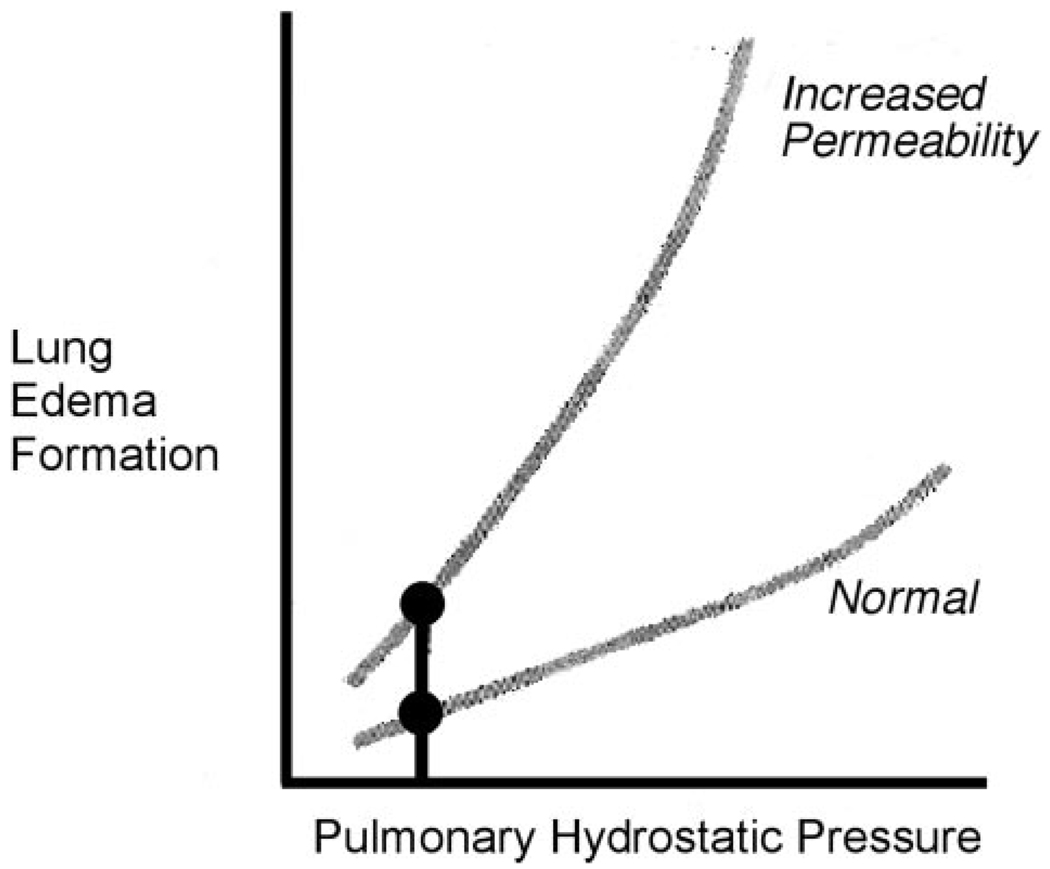
- Staub NC. Pulmonary edema: physiologic approaches to management. Chest. 1978;74:559–564. - PubMed
-
- Sakka SG, Klein M, Reinhart K, et al. Prognostic value of extravascular lung water in critically ill patients. Chest. 2002;122:2080–2086. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
