

Influence of race on inpatient treatment intensity at the end of life
- PMID: 17356965
- PMCID: PMC1824769
- DOI: 10.1007/s11606-006-0088-x
Influence of race on inpatient treatment intensity at the end of life
Abstract
Objective: To examine inpatient intensive care unit (ICU) and intensive procedure use by race among Medicare decedents, using utilization among survivors for comparison.
Design: Retrospective observational analysis of inpatient claims using multivariable hierarchical logistic regression.
Setting: United States, 1989-1999.
Participants: Hospitalized Medicare fee-for-service decedents (n = 976,220) and survivors (n = 845,306) aged 65 years or older.
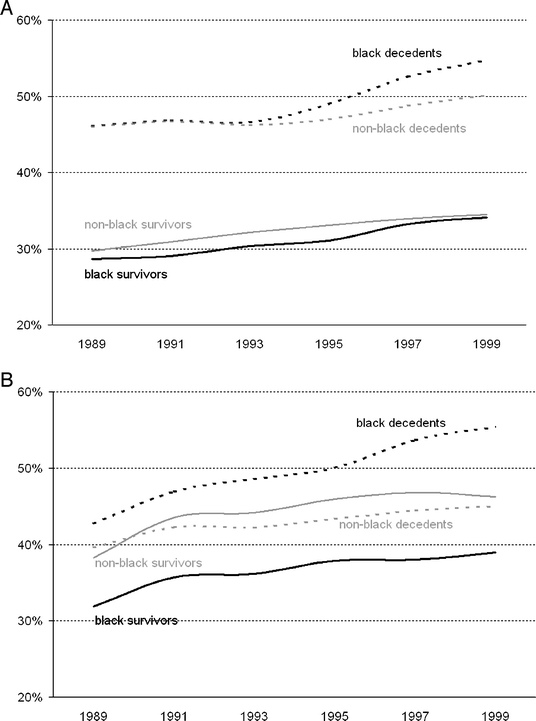
Measurements and main results: Admission to the ICU and use of one or more intensive procedures over 12 months, and, for inpatient decedents, during the terminal admission. Black decedents with one or more hospitalization in the last 12 months of life were slightly more likely than non-blacks to be admitted to the ICU during the last 12 months (49.3% vs. 47.4%, p <.0001) and the terminal hospitalization (41.9% vs. 40.6%, p < 0.0001), but these differences disappeared or attenuated in multivariable hierarchical logistic regressions (last 12 months adjusted odds ratio (AOR) 1.0 [0.99-1.03], p = .36; terminal hospitalization AOR 1.03 [1.0-1.06], p = .01). Black decedents were more likely to undergo an intensive procedure during the last 12 months (49.6% vs. 42.8%, p < .0001) and the terminal hospitalization (37.7% vs, 31.1%, p < .0001), a difference that persisted with adjustment (last 12 months AOR 1.1 [1.08-1.14], p < .0001; terminal hospitalization AOR 1.23 [1.20-1.26], p < .0001). Patterns of differences in inpatient treatment intensity by race were reversed among survivors: blacks had lower rates of ICU admission (31.2% vs. 32.4%, p < .0001; AOR 0.93 [0.91-0.95], p < .0001) and intensive procedure use (36.6% vs. 44.2%; AOR 0.72 [0.70-0.73], p <.0001). These differences were driven by greater use by blacks of life-sustaining treatments that predominate among decedents but lesser use of cardiovascular and orthopedic procedures that predominate among survivors. A hospital's black census was a strong predictor of inpatient end-of-life treatment intensity.
Conclusions: Black decedents were treated more intensively during hospitalization than non-black decedents, whereas black survivors were treated less intensively. These differences are strongly associated with a hospital's black census. The causes and consequences of these hospital-level differences in intensity deserve further study.
Figures
References
-
- Smedley B, Stith A, Nelson A, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academy Press: 2002. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
