

Physician practice patterns and variation in the delivery of preventive services
- PMID: 17356985
- PMCID: PMC1824741
- DOI: 10.1007/s11606-006-0042-y
Physician practice patterns and variation in the delivery of preventive services
Abstract
Background: Strategies to improve preventive services delivery (PSD) have yielded modest effects. A multidimensional approach that examines distinctive configurations of physician attributes, practice processes, and contextual factors may be informative in understanding delivery of this important form of care.
Objective: We identified naturally occurring configurations of physician practice characteristics (PPCs) and assessed their association with PSD, including variation within configurations.
Design: Cross-sectional study.
Participants: One hundred thirty-eight family physicians in 84 community practices and 4,046 outpatient visits.
Measurements: Physician knowledge, attitudes, use of tools and staff, and practice patterns were assessed by ethnographic and survey methods. PSD was assessed using direct observation of the visit and medical record review. Cluster analysis identified unique configurations of PPCs. A priori hypotheses of the configurations likely to perform the best on PSD were tested using a multilevel random effects model.
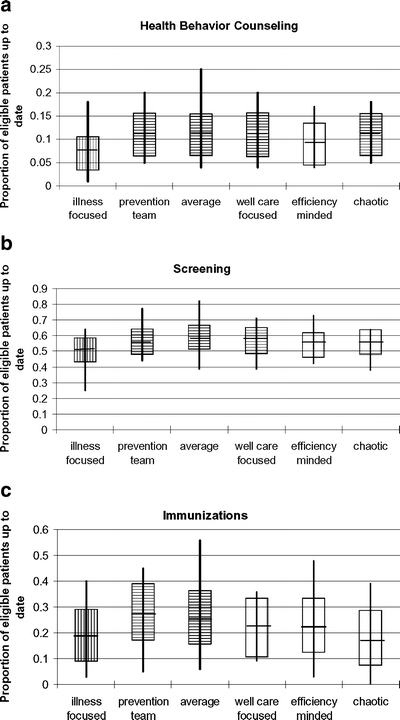
Results: Six distinct PPC configurations were identified. Although PSD significantly differed across configurations, mean differences between configurations with the lowest and highest PSD were small (i.e., 3.4, 7.7, and 10.8 points for health behavior counseling, screening, and immunizations, respectively, on a 100-point scale). Hypotheses were not confirmed. Considerable variation of PSD rates within configurations was observed.
Conclusions: Similar rates of PSD can be attained through diverse physician practice configurations. Significant within-configuration variation may reflect dynamic interactions between PPCs as well as between these characteristics and the contexts in which physicians function. Striving for a single ideal configuration may be less valuable for improving PSD than understanding and leveraging existing characteristics within primary care practices.
Figures
Similar articles
-
Does patient educational level affect office visits to family physicians?J Natl Med Assoc. 2002 Mar;94(3):157-65. J Natl Med Assoc. 2002. PMID: 11918385 Free PMC article.
-
Tools, teamwork, and tenacity: an examination of family practice office system influences on preventive service delivery.Prev Med. 2003 Feb;36(2):131-40. doi: 10.1016/s0091-7435(02)00024-5. Prev Med. 2003. PMID: 12590987
-
Delivery of preventive services to older adults by primary care physicians.JAMA. 2005 Jul 27;294(4):473-81. doi: 10.1001/jama.294.4.473. JAMA. 2005. PMID: 16046654
-
The value of a family physician.J Fam Pract. 1998 May;46(5):363-8. J Fam Pract. 1998. PMID: 9597993 Review.
-
Office-based interventions to improve delivery of cancer prevention services by primary care physicians.Cancer. 1993 Aug 1;72(3 Suppl):1100-12. doi: 10.1002/1097-0142(19930801)72:3+<1100::aid-cncr2820721327>3.0.co;2-n. Cancer. 1993. PMID: 8334665 Review.
Cited by
-
Does Receiving Clinical Preventive Services Vary across Different Types of Primary Healthcare Organizations? Evidence from a Population-Based Survey.Healthc Policy. 2010 Nov;6(2):67-84. Healthc Policy. 2010. PMID: 22043224 Free PMC article.
-
Evaluation of the effect of decision support on the efficiency of primary care providers in the outpatient practice.J Prim Care Community Health. 2015 Jan;6(1):54-60. doi: 10.1177/2150131914546325. Epub 2014 Aug 25. J Prim Care Community Health. 2015. PMID: 25155103 Free PMC article. Clinical Trial.
-
Knowledge, attitudes, and practice patterns of recurrent urinary stones prevention in Saudi Arabia.Urolithiasis. 2016 Apr;44(2):135-43. doi: 10.1007/s00240-015-0815-z. Epub 2015 Aug 22. Urolithiasis. 2016. PMID: 26296383
-
Cognitive testing in older primary care patients: A cluster-randomized trial.Alzheimers Dement (Amst). 2015 Sep 1;1(3):349-357. doi: 10.1016/j.dadm.2015.06.009. Alzheimers Dement (Amst). 2015. PMID: 26380844 Free PMC article.
-
Impact of an educational intervention designed to reduce unnecessary recall during screening mammography.Acad Radiol. 2012 Sep;19(9):1114-20. doi: 10.1016/j.acra.2012.05.003. Epub 2012 Jun 23. Acad Radiol. 2012. PMID: 22727623 Free PMC article. Clinical Trial.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PMC', 'value': 'PMC1615482', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1615482/'}, {'type': 'PubMed', 'value': '7762721', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/7762721/'}]}
- Anderson L, May DS. Has the use of cervical, breast, and colorectal cancer screening increased in the United States? Am J Public Health. 1995;85:840–2. - PMC - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9179135', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9179135/'}]}
- Kottke TE, Solberg LI, Brekke ML, Cabrera A, Marquez MA. Delivery rates for preventive services in 44 Midwestern clinics. Mayo Clin Proc. 1997;72(6):515–23. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1006/pmed.2000.0700', 'is_inner': False, 'url': 'https://doi.org/10.1006/pmed.2000.0700'}, {'type': 'PubMed', 'value': '10938218', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10938218/'}]}
- Stange KC, Flocke SA, Goodwin MA, Kelly RB, Zyzanski SJ. Direct observation of rates of preventive service delivery in community family practice. Prev Med. 2000;31:167–76. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1001/jama.282.15.1458', 'is_inner': False, 'url': 'https://doi.org/10.1001/jama.282.15.1458'}, {'type': 'PubMed', 'value': '10535437', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10535437/'}]}
- Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282(15):1458–65. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1006/pmed.1998.0337', 'is_inner': False, 'url': 'https://doi.org/10.1006/pmed.1998.0337'}, {'type': 'PubMed', 'value': '9672958', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9672958/'}]}
- Solberg LI, Kottke TE, Brekke ML. Will primary care clinics organize themselves to improve the delivery of preventive services? A randomized controlled trial. Prev Med. 1998;27(4):623–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
