

Use of serological assays for diagnosis of hepatitis E virus genotype 1 and 3 infections in a setting of low endemicity
- PMID: 17360853
- PMCID: PMC1865643
- DOI: 10.1128/CVI.00231-06
Use of serological assays for diagnosis of hepatitis E virus genotype 1 and 3 infections in a setting of low endemicity
Abstract
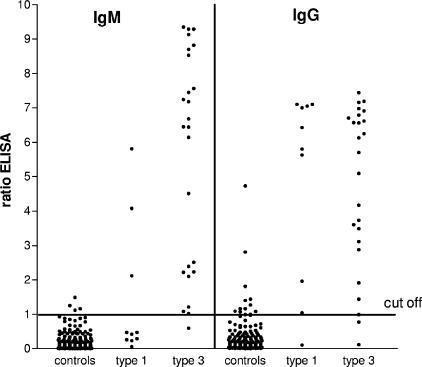
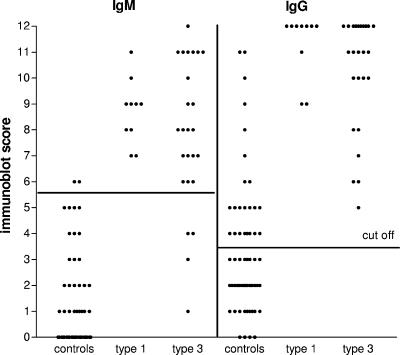
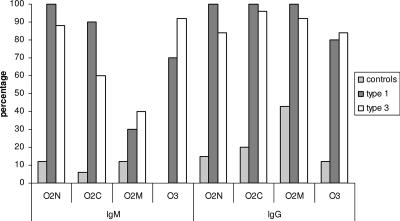
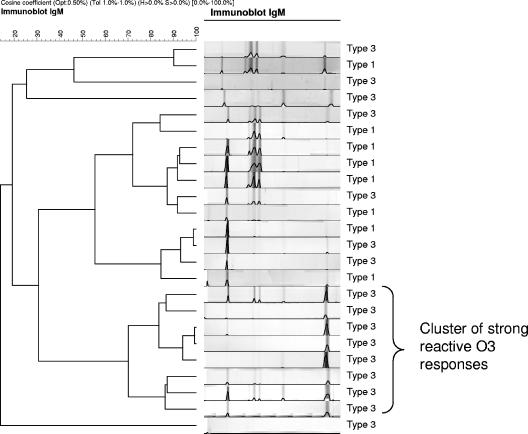
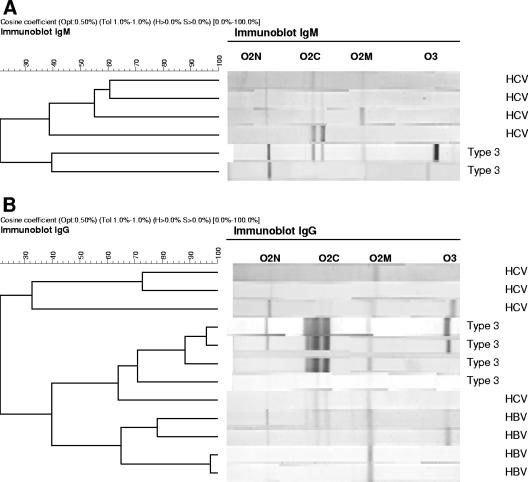
Because of the occurrence of genotype 3 hepatitis E virus (HEV) in regions of low endemicity, it is important to validate the currently used serological assays for diagnosing infections with viruses belonging to this lineage, since these assays only use antigens derived from genotype 1 and 2 viruses. We evaluated the Genelabs enzyme-linked immunosorbent assay (ELISA) and the RecomBlot from Mikrogen for the detection of HEV-specific immunoglobulin M (IgM) and IgG under conditions of low endemicity. We compared test results of 16 patients with locally acquired genotype 3 HEV, 8 genotype 1 patients, 167 healthy controls from the general population, and 101 cases with hepatitis due to other viral causes. The measured specificities of the ELISA (98%) and the RecomBlot (97%) were comparable to those given by the manufacturer for IgM but were significantly lower for IgG (93% by ELISA and 66% by immunoblotting, versus reported values of 98% for ELISA and 95% for blotting). Antibody levels detected following infections with genotype 3 were lower than those following genotype 1 infections except for those measured in the IgM ELISA. Reactivity to the four antigens used in the immunoblot assay were analyzed and showed differences in the IgM immunoblot reactions between genotype 1 patients and genotype 3 patients. The ORF3 antigen was the most specific antigen. The specificity could be improved by a combined testing regimen with confirmation by immunoblotting of all positive ELISA results and by raising the cutoff of the IgG immunoblot assay without loss of sensitivity. We conclude that a combination of ELISA and immunoblotting is needed for acceptable specificity and sensitivity of HEV assays under conditions of low endemicity.
Figures
References
-
- Aggarwal, R., and S. R. Naik. 1997. Epidemiology of hepatitis E: past, present and future. Trop. Gastroenterol. 18:49-56. - PubMed
-
- Balayan, M. S., A. G. Andjaparidze, S. S. Savinsaya, E. S. Ketiladze, D. M. Braginsky, A. P. Savinov, and V. F. Poleschuk. 1983. Evidence for a virus in non-A, non-B hepatitis transmitted via the fecal-oral route. Intervirology 20:23-31. - PubMed
-
- Colac, D., D. Ogunc, F. Gunseren, S. Velipasaoglu, M. R. Aktekin, and M. Gultekin. 2002. Seroprevalence of antibodies to hepatitis A and E viruses in pediatric age groups in turkey. Acta Microbiol. Immunol. Hung. 49:93-97. - PubMed
-
- Corwin, A. L., H. B. Khiem, E. T. Clayson, K. S. Pham, T. T. Vo, T. Y. Vu, T. T. Cao, D. Vaughn, J. Merven, T. L. Richie, M. P. Putri, J. He, R. Graham, F. S. Wignall, and K. C. Hyams. 1996. A waterborne outbreak of hepatitis E virus transmission in south-western Vietnam. Am. J. Trop. Med. Hyg. 54:559-562. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
