

Indian community health insurance schemes provide partial protection against catastrophic health expenditure
- PMID: 17362506
- PMCID: PMC1852553
- DOI: 10.1186/1472-6963-7-43
Indian community health insurance schemes provide partial protection against catastrophic health expenditure
Abstract
Background: More than 72% of health expenditure in India is financed by individual households at the time of illness through out-of-pocket payments. This is a highly regressive way of financing health care and sometimes leads to impoverishment. Health insurance is recommended as a measure to protect households from such catastrophic health expenditure (CHE). We studied two Indian community health insurance (CHI) schemes, ACCORD and SEWA, to determine whether insured households are protected from CHE.
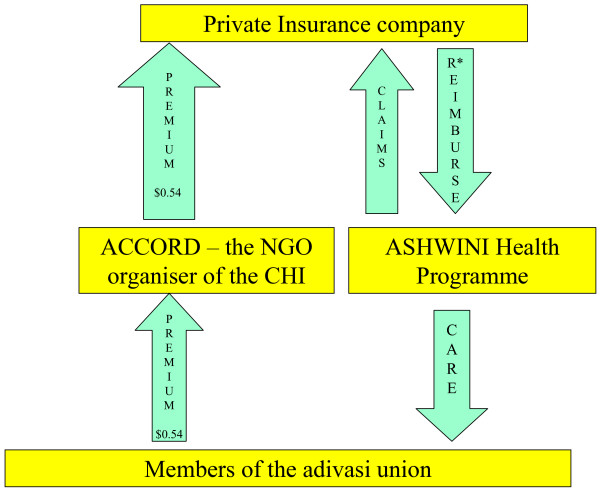
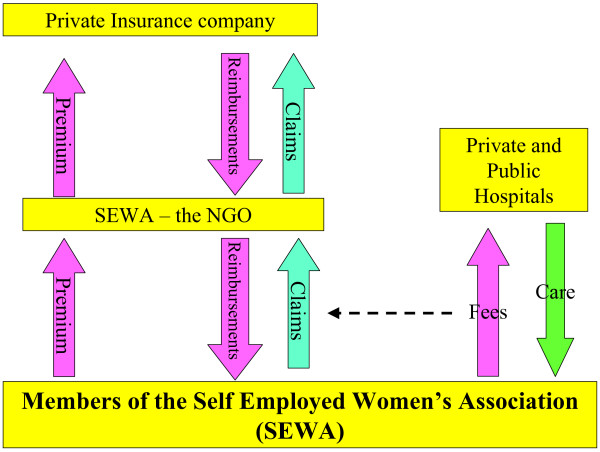
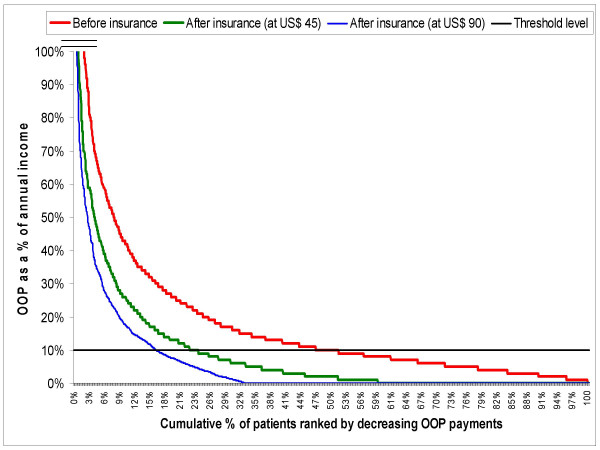
Methods: ACCORD provides health insurance cover for the indigenous population, living in Gudalur, Tamil Nadu. SEWA provides insurance cover for self employed women in the state of Gujarat. Both cover hospitalisation expenses, but only upto a maximum limit of US$23 and US$45, respectively. We reviewed the insurance claims registers in both schemes and identified patients who were hospitalised during the period 01/04/2003 to 31/03/2004. Details of their diagnoses, places and costs of treatment and self-reported annual incomes were obtained. There is no single definition of CHE and none of these have been validated. For this research, we used the following definition; "annual hospital expenditure greater than 10% of annual income," to identify those who experienced CHE.
Results: There were a total of 683 and 3152 hospital admissions at ACCORD and SEWA, respectively. In the absence of the CHI scheme, all of the patients at ACCORD and SEWA would have had to pay OOP for their hospitalisation. With the CHI scheme, 67% and 34% of patients did not have to make any out-of-pocket (OOP) payment for their hospital expenses at ACCORD and SEWA, respectively. Both CHI schemes halved the number of households that would have experienced CHE by covering hospital costs. However, despite this, 4% and 23% of households with admissions still experienced CHE at ACCORD and SEWA, respectively. This was related to the following conditions: low annual income, benefit packages with low maximum limits, exclusion of some conditions from the benefit package, and use of the private sector for admissions.
Conclusion: CHI appears to be effective at halving the incidence of CHE among hospitalised patients. This protection could be further enhanced by improving the design of the CHI schemes, especially by increasing the upper limits of benefit packages, minimising exclusions and controlling costs.
Figures
References
-
- Ministry of Health & Family Welfare . National Health Accounts, India. New Delhi: Government of India; 2006.
-
- WHO . The world health report 2006 – working together for health. Geneva: WHO; 2006. - PubMed
-
- Garg CC, Karan AK. Health and Millennium Development Goal 1: Reducing out-of-pocket expenditures to reduce income poverty – Evidence from India. Manila: Equitap; 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
