

A nasal cannula can be used to treat obstructive sleep apnea
- PMID: 17363769
- PMCID: PMC1994212
- DOI: 10.1164/rccm.200609-1336OC
A nasal cannula can be used to treat obstructive sleep apnea
Abstract
Rationale: Obstructive sleep apnea syndrome is due to upper airway obstruction and is associated with increased morbidity. Although continuous positive airway pressure efficaciously treats obstructive apneas and hypopneas, treatment is impeded by low adherence rates.
Objectives: To assess the efficacy on obstructive sleep apnea of a minimally intrusive method for delivering warm and humidified air through an open nasal cannula.
Methods: Eleven subjects (age, 49.7+/-5.0 yr; body mass index, 30.5+/-4.3 kg/m2), with obstructive apnea-hypopnea syndrome ranging from mild to severe (5 to 60 events/h), were administered warm and humidified air at 20 L/minute through an open nasal cannula.
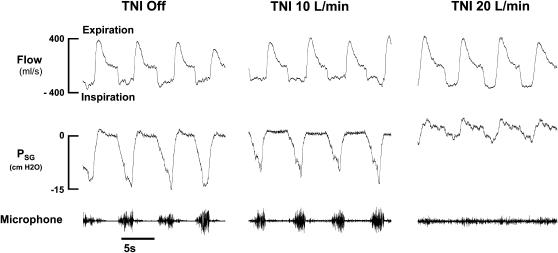
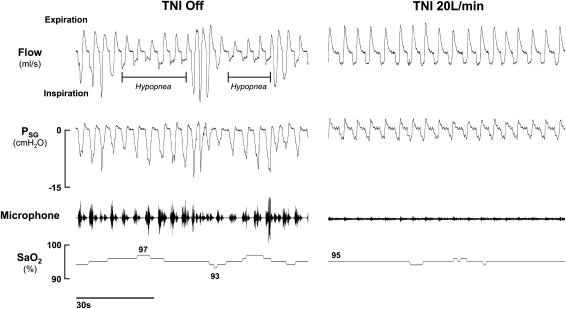
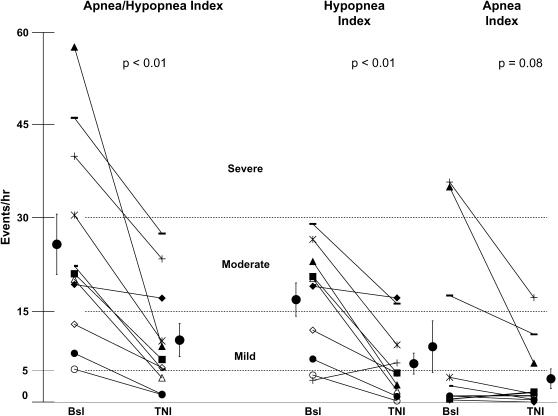
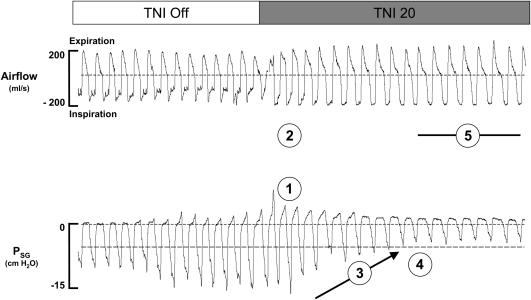
Measurements and main results: Measurements were based on standard sleep-disordered breathing and arousal indices. In a subset of patients pharyngeal pressure and ventilation were assessed to determine the mechanism of action of treatment with nasal insufflation. Treatment with nasal insufflation reduced the mean apnea-hypopnea index from 28+/-5 to 10+/-3 events per hour (p<0.01), and reduced the respiratory arousal index from 18+/-2 to 8+/-2 events per hour (p<0.01). Treatment with nasal insufflation reduced the apnea-hypopnea index to fewer than 10 events per hour in 8 of 11 subjects, and to fewer than 5 events per hour in 4 subjects. The mechanism of action appears to be through an increase in end-expiratory pharyngeal pressure, which alleviated upper airway obstruction and improved ventilation.
Conclusions: Our findings demonstrate clinical proof of concept that a nasal cannula for insufflating high airflows can be used to treat a diverse group of patients with obstructive sleep apnea.
Figures

References
-
- Babu AR, Herdegen J, Fogelfeld L, Shott S, Mazzone T. Type 2 diabetes, glycemic control, and continuous positive airway pressure in obstructive sleep apnea. Arch Intern Med 2005;165:447–452. - PubMed
-
- Punjabi NM, Shahar E, Redline S, Golttlieb DJ, Givelber R, Resnick HE. Sleep-disordered breathing, glucose intolerance, and insulin resistance: the Sleep Heart Health Study. Am J Epidemiol 2004;160:521–530. - PubMed
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea–hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365:1046–1053. - PubMed
-
- Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005;353:2034–2041. - PubMed
-
- Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981;1(8225):862–865. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
