

What is new in otitis media?
- PMID: 17364173
- PMCID: PMC1876255
- DOI: 10.1007/s00431-007-0461-8
What is new in otitis media?
Abstract
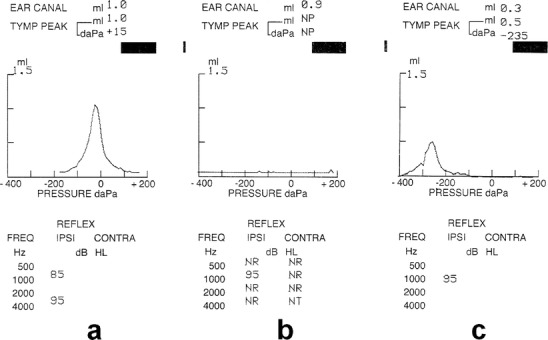
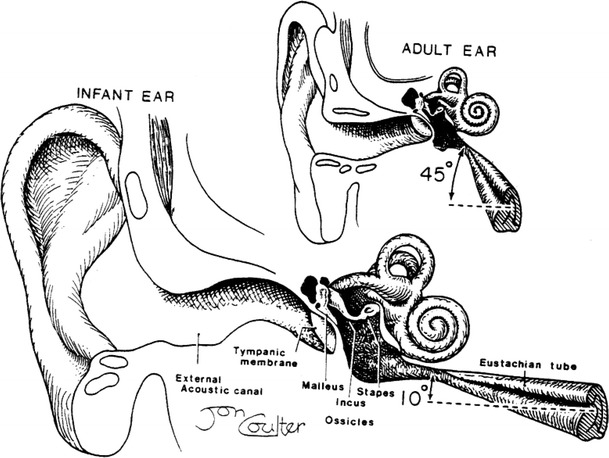
The "wait and see" approach in acute otitis media (AOM), consisting of postponing the antibiotic administration for a few days, has been advocated mainly to counteract the increased bacterial resistance in respiratory infections. This approach is not justified in children less than 2 years of age and this for several reasons. First, AOM is an acute inflammation of the middle ear caused in about 70% of cases by bacteria. Redness and bulging of the tympanic membrane are characteristic findings in bacterial AOM. Second, AOM is associated with long-term dysfunction of the inflamed eustachian tube (ET), particularly in children less than 2 years of age. In this age group, the small calibre of the ET together with its horizontal direction result in impaired clearance, ventilation and protection of the middle ear. Third, recent prospective studies have shown poor long-term prognosis of AOM in children below 2 years with at least 50% of recurrences and persisting otitis media with effusion (OME) in about 35% 6 months after AOM. Viruses elicit AOM in about 30% of children. A prolonged course of AOM has been observed when bacterial and viral infections are combined because viral infection is also associated with ET dysfunction in young children. Bacterial and viral testing of the nasopharyngeal aspirate is an excellent tool both for initial treatment and recurrence of AOM. Antibiotic treatment of AOM is mandatory in children less than 2 years of age to decrease inflammation in the middle ear but also of the ET particularly during the first episode. The best choice is amoxicillin because of its superior penetration in the middle ear. Streptococci pneumoniae with intermediary bacterial resistance to penicillin are particularly associated with recurrent AOM. Therefore the dosage of amoxicillin should be 90 mg/kg per day in three doses. In recurrent AOM with beta-lactamase-producing bacilli, amoxicillin should be associated with clavulanic acid at a dose of 6.4 mg/kg per day. The duration of the treatment is not established yet but 10 days is reasonable for a first episode of AOM. OME may be a precursor initiating AOM but also a complication thereof. OME needs a watchful waiting approach. When associated with deafness for 2-3 months in children over 2 years of age, an antibiotic should be given according to the results of the bacterial resistance in the nasopharyngeal aspirate. The high rate of complications of tympanostomy tube insertion outweighs the beneficial effect on hearing loss. The poor results of this procedure are due to the absence of effects on ET dysfunction. Pneumococcal vaccination has little beneficial effects on recurrent AOM and its use in infants needs further studies. Treatment with amoxicillin is indicated in all children younger than 2 years with a first episode of AOM presenting with redness and bulging of the tympanic membrane. Combined amoxicillin and clavulanic acid should be given in patients with beta-lactamase-producing bacteria. The duration of treatment is estimated to be at least 10 days depending on the findings by pneumo-otoscopy and tympanometry. Bacterial and viral testing of the nasopharyngeal aspirate is highly recommended particularly in children in day care centres as well as for regular follow-up. The high recurrence rate is due to the long-lasting dysfunction of the eustachian tube and the immune immaturity of children less than 2 years of age.
Figures


Similar articles
-
Clinical practice guideline: Tympanostomy tubes in children.Otolaryngol Head Neck Surg. 2013 Jul;149(1 Suppl):S1-35. doi: 10.1177/0194599813487302. Otolaryngol Head Neck Surg. 2013. PMID: 23818543
-
Efficacy of 20- versus 10-day antimicrobial treatment for acute otitis media.Pediatrics. 1995 Jul;96(1 Pt 1):5-13. Pediatrics. 1995. PMID: 7596722 Clinical Trial.
-
Recurrent acute otitis media occurring within one month from completion of antibiotic therapy: relationship to the original pathogen.Pediatr Infect Dis J. 2003 Mar;22(3):209-16. doi: 10.1097/01.inf.0000066798.69778.07. Pediatr Infect Dis J. 2003. PMID: 12634580
-
Acute otitis media disease management.Minerva Pediatr. 2003 Oct;55(5):415-38. Minerva Pediatr. 2003. PMID: 14608265 Review.
-
Medical management of middle ear disease in children less than 2 years of age with sensorineural hearing loss.J Otolaryngol. 2005 Aug;34 Suppl 2:S64-9. J Otolaryngol. 2005. PMID: 16076419 Review.
Cited by
-
Inhibition of lipopolysaccharide-induced inflammation by trophoblast-conditioned medium and trophoblast-derived extracellular vesicles in human middle ear epithelial cells.Sci Rep. 2023 Nov 14;13(1):19822. doi: 10.1038/s41598-023-46731-7. Sci Rep. 2023. PMID: 37963902 Free PMC article.
-
Role of a proprietary propolis-based product on the wait-and-see approach in acute otitis media and in preventing evolution to tracheitis, bronchitis, or rhinosinusitis from nonstreptococcal pharyngitis.Int J Gen Med. 2016 Nov 11;9:409-414. doi: 10.2147/IJGM.S118967. eCollection 2016. Int J Gen Med. 2016. PMID: 27956842 Free PMC article.
-
Cholinergic chemosensory cells in the auditory tube.Histochem Cell Biol. 2012 Apr;137(4):483-97. doi: 10.1007/s00418-012-0911-x. Epub 2012 Jan 20. Histochem Cell Biol. 2012. PMID: 22261922
-
Otoacoustic Emissions in Children with Long-Term Middle Ear Disease.Life (Basel). 2020 Nov 18;10(11):287. doi: 10.3390/life10110287. Life (Basel). 2020. PMID: 33217895 Free PMC article.
-
Societal costs and burden of otitis media in Portugal.J Multidiscip Healthc. 2011 Apr 4;4:53-62. doi: 10.2147/JMDH.S17529. J Multidiscip Healthc. 2011. PMID: 21544248 Free PMC article.
References
-
- Bluestone CD, Klein JO. Otitis media with effusion, atelectasis, and Eustachian tube dysfunction. In: Bluestone CD, Stool SE, editors. Pediatric otolaryngology. Philadelphia: Saunders; 1983. pp. 356–512.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
