

Why did outbreaks of severe acute respiratory syndrome occur in some hospital wards but not in others?
- PMID: 17366443
- PMCID: PMC7107862
- DOI: 10.1086/512819
Why did outbreaks of severe acute respiratory syndrome occur in some hospital wards but not in others?
Abstract
Background: Most documented "superspreading events" of severe acute respiratory syndrome (SARS) occurred in hospitals, but the underlying causes remain unclear. We systematically analyzed the risk factors for nosocomial outbreaks of SARS among hospital wards in Guangzhou and Hong Kong, China.
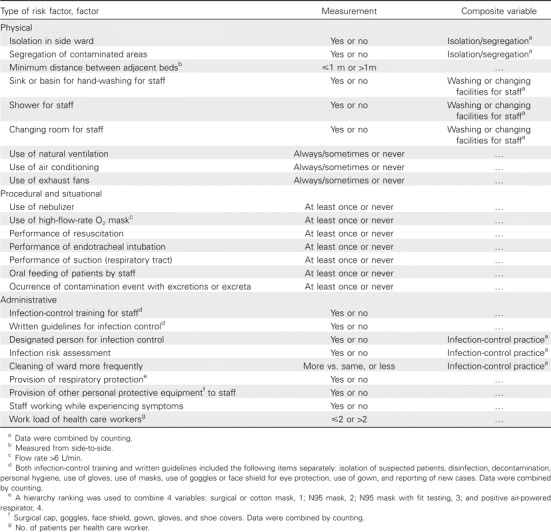
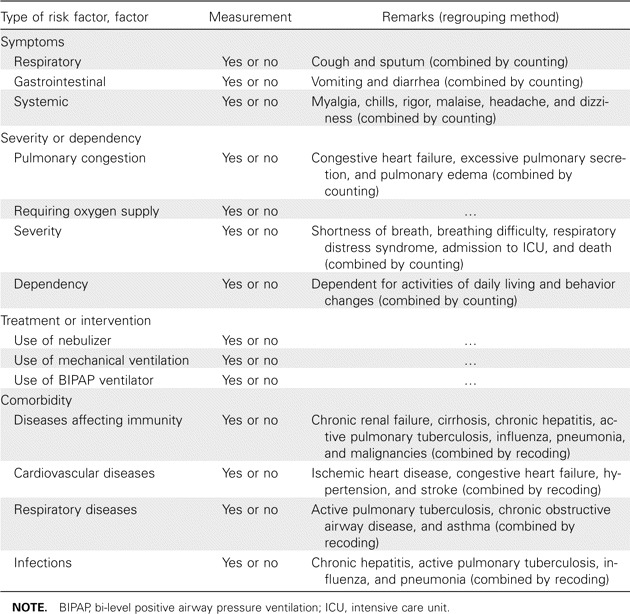
Methods: A case-control study was conducted. Case wards were hospital wards in which superspreading events of SARS occurred, and control wards were wards in which patients with SARS were admitted, but no subsequent nosocomial outbreaks occurred. Information on environmental and administrative factors was obtained through visits to the wards and interviews with ward managers or nursing officers. Relevant information about host factors was abstracted from the medical records. Logistic regression analyses were used to identify the major risk factors for superspreading events.
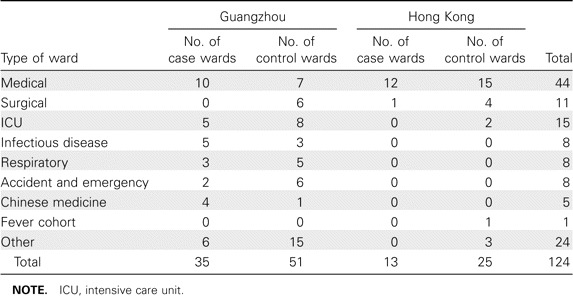
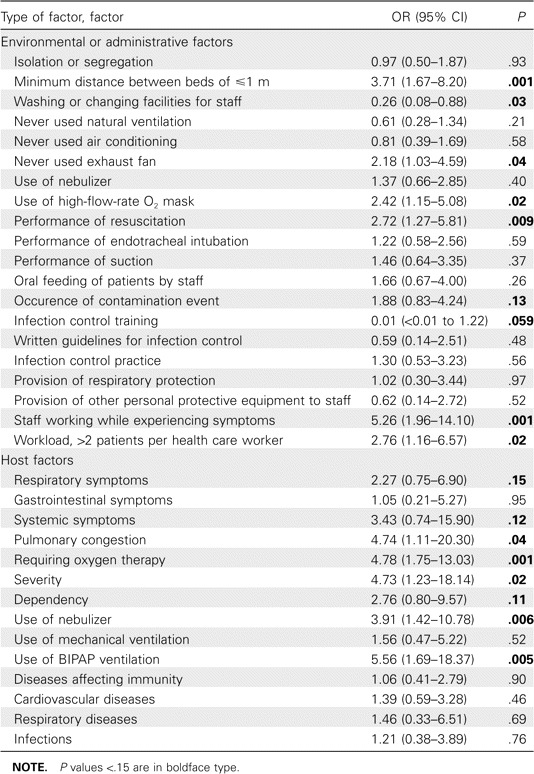
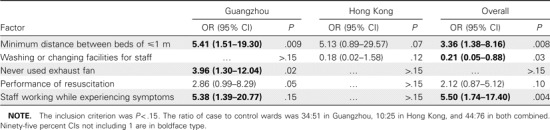
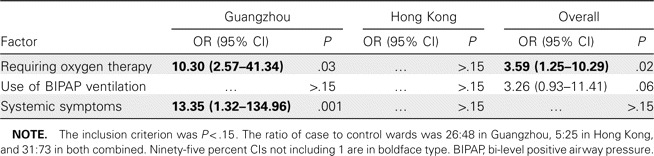
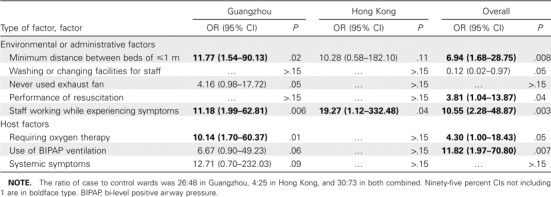
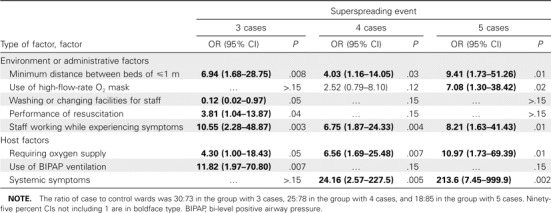
Results: Eighty-six wards in 21 hospitals in Guangzhou and 38 wards in 5 hospitals in Hong Kong were included in the study. Six risk factors were significant in the final multiple-logistic regression model: minimum distance between beds of < or = 1 m (odds ratio [OR], 6.94; 95% confidence interval [CI], 1.68-28.75), availability of washing or changing facilities for staff (OR, 0.12; 95% CI, 0.02-0.97), whether resuscitation was ever performed in the ward (OR, 3.81; 95% CI, 1.04-13.87), whether staff members worked while experiencing symptoms (OR, 10.55; 95% CI, 2.28-48.87), whether any host patients (index patient or the first patient with SARS admitted to a ward) required oxygen therapy (OR, 4.30; 95% CI, 1.00-18.43), and whether any host patients required bi-level positive airway pressure ventilation (OR, 11.82; 95% CI, 1.97-70.80).
Conclusions: Our results revealed that factors that were associated with the ward environment and administration were important in nosocomial outbreaks of SARS. The lessons learned from this study remain very important and highly relevant to the daily operation of hospital wards if we are to prevent nosocomial outbreaks of other respiratory infections in the future.
Figures
Comment in
-
Nosocomial transmission of severe acute respiratory syndrome: better quality of evidence is needed.Clin Infect Dis. 2007 Dec 15;45(12):1651; author reply 1652. doi: 10.1086/523725. Clin Infect Dis. 2007. PMID: 18190333 No abstract available.
References
-
- Centers for Disease Control and Prevention. Update: outbreak of severe acute respiratory syndrome: worldwide, 2003. MMWR Morb Mortal Wkly Rep. 2003;52:241–6. 248. - PubMed
-
- World Health Organization. Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003. Revised 26 September 2003. Available at: http://www.who.int/csr/sars/country/table2003_09_23/en/. Accessed 22 June 2006.
-
- Yu ITS, Li Y, Wong TW, et al. Evidence of airborne transmission of the severe acute respiratory syndrome virus. N Engl J Med. 2004;350:1731–9. - PubMed
-
- World Health Organization. 2003. Severe acute respiratory syndrome (SARS)-multi-country outbreak: update 30: status of diagnostic test, significance of “super spreaders,” situation in China. Available at: http://www.who.int/csr/don/2003_04_15/en/. Accessed 22 June 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
