

Dihydroartemisinin-piperaquine versus artesunate-amodiaquine: superior efficacy and posttreatment prophylaxis against multidrug-resistant Plasmodium falciparum and Plasmodium vivax malaria
- PMID: 17366451
- PMCID: PMC2532501
- DOI: 10.1086/512677
Dihydroartemisinin-piperaquine versus artesunate-amodiaquine: superior efficacy and posttreatment prophylaxis against multidrug-resistant Plasmodium falciparum and Plasmodium vivax malaria
Abstract
Background: Antimalarial drug resistance is now well established in both Plasmodium falciparum and Plasmodium vivax. In southern Papua, Indonesia, where both strains of plasmodia coexist, we have been conducting a series of studies to optimize treatment strategies.
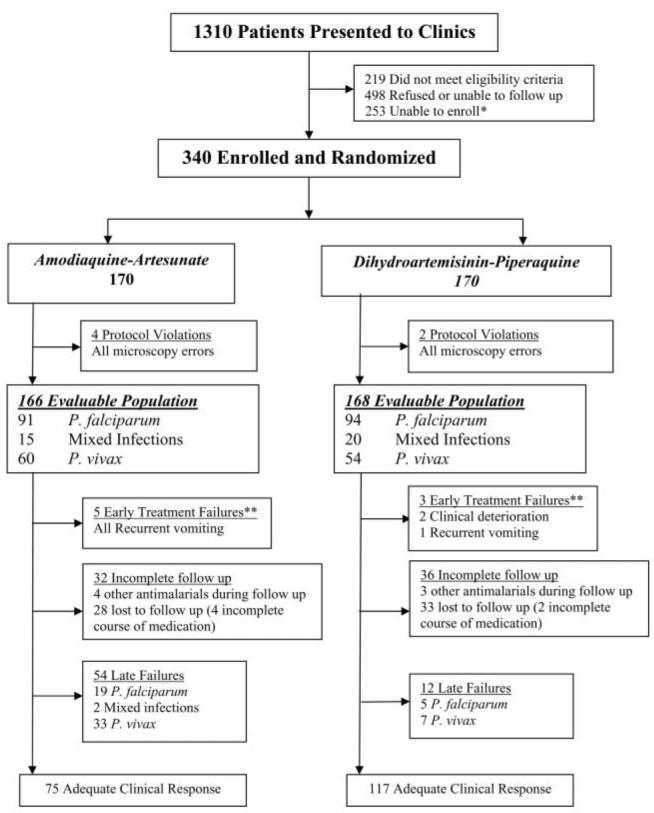
Methods: We conducted a randomized trial that compared the efficacy and safety of dihydroartemisinin-piperaquine (DHP) with artesunate-amodiaquine (AAQ). The primary end point was the overall cumulative parasitological failure rate at day 42.
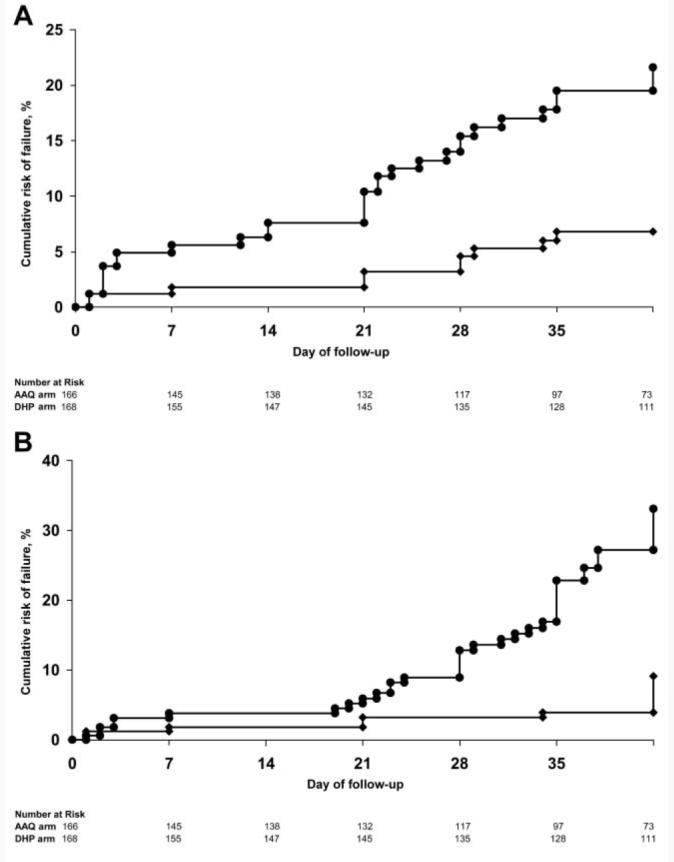
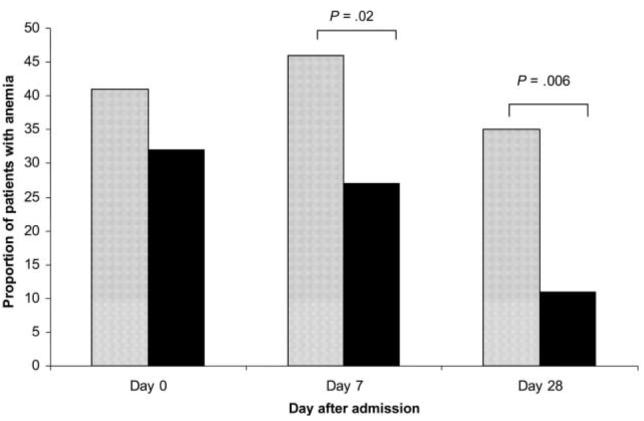
Results: Of the 334 patients in the evaluable patient population, 185 were infected with P. falciparum, 80 were infected with P. vivax, and 69 were infected with both species. The overall parasitological failure rate at day 42 was 45% (95% confidence interval [CI], 36%-53%) for AAQ and 13% (95% CI, 7.2%-19%) for DHP (hazard ratio [HR], 4.3; 95% CI, 2.5-7.2; P<.001). Rates of both recrudescence of P. falciparum infection and recurrence of P. vivax infection were significantly higher after receipt of AAQ than after receipt of DHP (HR, 3.4 [95% CI, 1.2-9.4] and 4.3 [95% CI, 2.2-8.2], respectively; P<.001). By the end of the study, AAQ recipients were 2.95-fold (95% CI, 1.2- to 4.9-fold) more likely to be anemic and 14.5-fold (95% CI, 3.4- to 61-fold) more likely to have carried P. vivax gametocytes.
Conclusions: DHP was more effective and better tolerated than AAQ against multidrug-resistant P. falciparum and P. vivax infections. The prolonged therapeutic effect of piperaquine delayed the time to P. falciparum reinfection, decreased the rate of recurrence of P. vivax infection, and reduced the risk of P. vivax gametocyte carriage and anemia.
Figures
Comment in
-
Combination therapy for malaria: mission accomplished?Clin Infect Dis. 2007 Apr 15;44(8):1075-7. doi: 10.1086/512743. Epub 2007 Mar 5. Clin Infect Dis. 2007. PMID: 17366452 No abstract available.
References
-
- Rieckmann KH, Davis DR, Hutton DC. Plasmodium vivax resistance to chloroquine? Lancet. 1989;2:1183–4. - PubMed
-
- Baird JK, Basri H, et al. Resistance to chloroquine by Plasmodium vivax in Irian Jaya, Indonesia. Am J Trop Med Hyg. 1991;44:547–52. - PubMed
-
- Baird JK, Sustriayu Nalim MF, Basri H, et al. Survey of resistance to chloroquine by Plasmodium vivax in Indonesia. Trans R Soc Trop Med Hyg. 1996;90:409–11. - PubMed
-
- Marlar T, Myat Phone K, Aye Yu S, Khaing Khaing G, Ma S, Myint O. Development of resistance to chloroquine by Plasmodium vivax in Myanmar. Trans R Soc Trop Med Hyg. 1995;89:307–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
