

Pleural and pericardial effusion: a potential ultrasonographic marker for the prenatal differential diagnosis between congenital diaphragmatic eventration and congenital diaphragmatic hernia
- PMID: 17366518
- PMCID: PMC2391071
- DOI: 10.1002/uog.3958
Pleural and pericardial effusion: a potential ultrasonographic marker for the prenatal differential diagnosis between congenital diaphragmatic eventration and congenital diaphragmatic hernia
Abstract
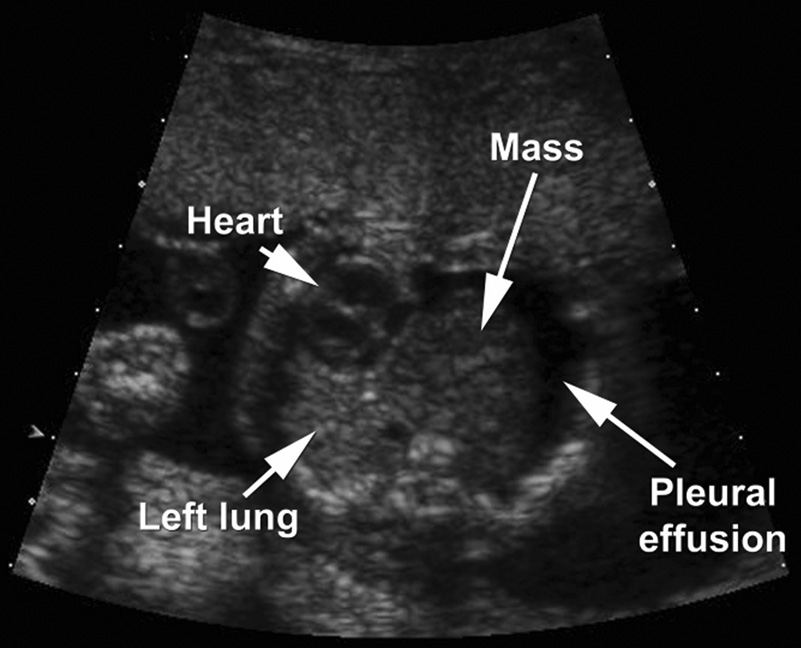
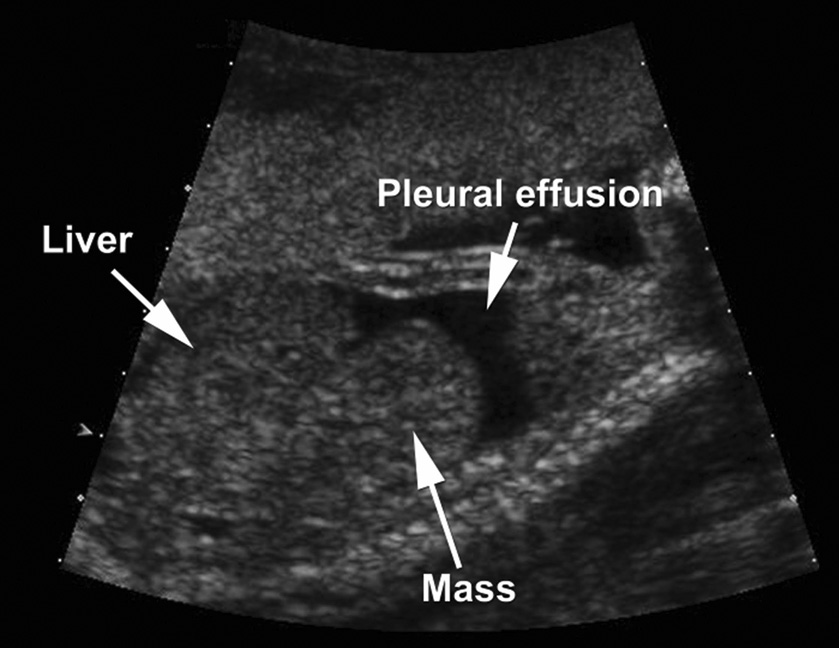
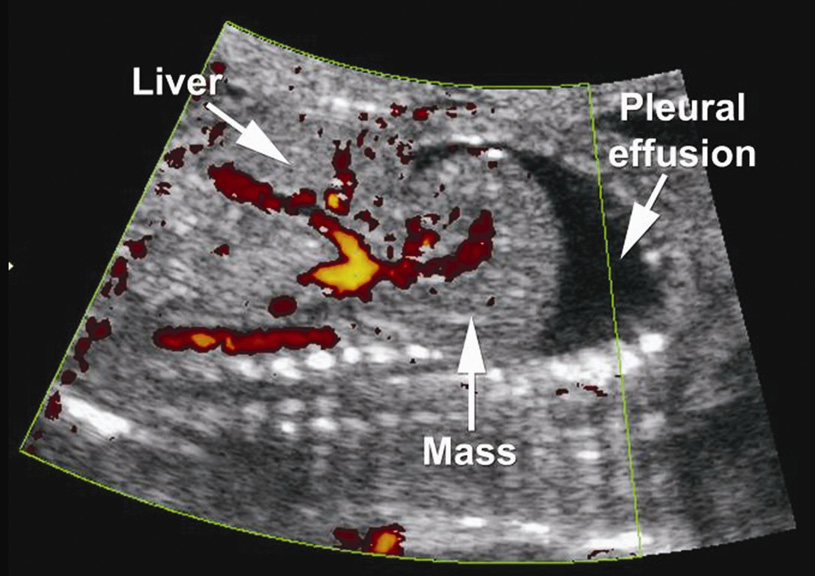
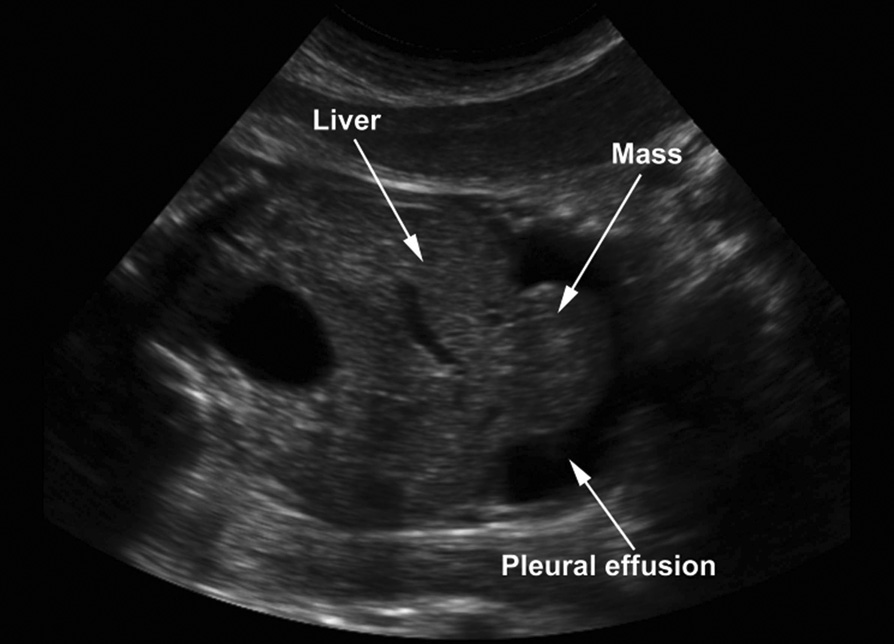
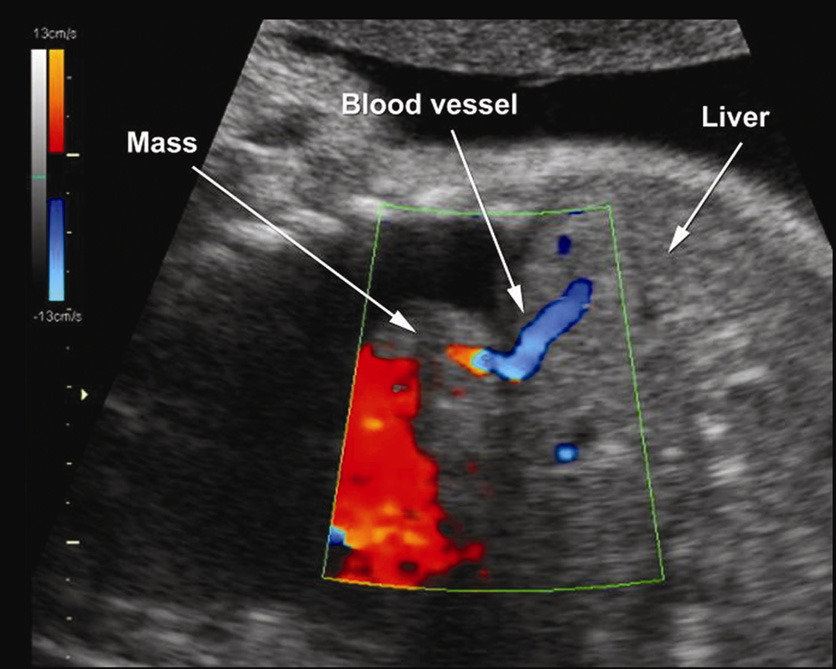
Objectives: To determine whether or not the presence of pleural and/or pericardial effusion can be used prenatally as an ultrasonographic marker for the differential diagnosis between diaphragmatic eventration and diaphragmatic hernia.
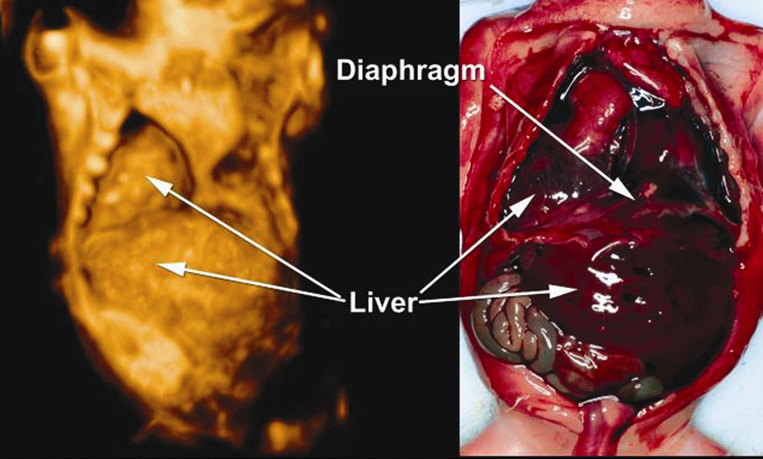
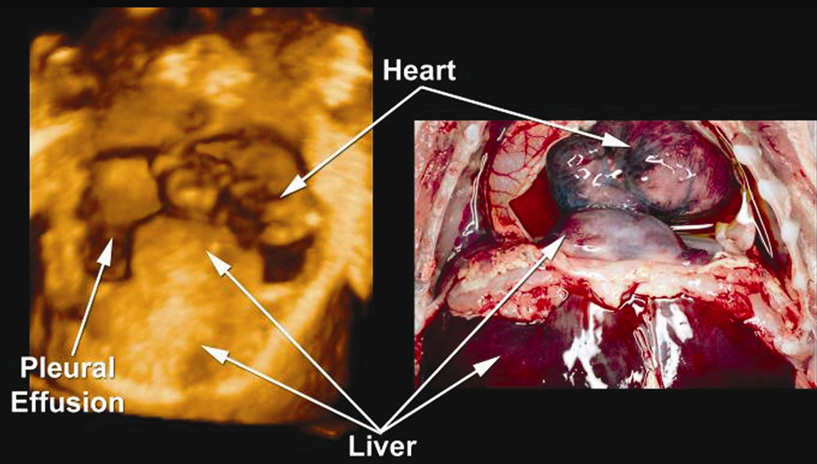
Methods: We present two case reports of non-isolated diaphragmatic eventration associated with pleural and/or pericardial effusion. Additionally, we reviewed the literature for all cases of congenital diaphragmatic hernia (CDH) and diaphragmatic eventration that met the following criteria: (1) prenatal diagnosis of a diaphragmatic defect and (2) definitive diagnosis by autopsy or surgery. The frequencies of pleural effusion, pericardial effusion and hydrops were compared between the two conditions using Fisher's exact test. A subanalysis was conducted of cases with isolated diaphragmatic defects (i.e. diaphragmatic defects not associated with hydrops and other major structural or chromosomal anomalies).
Results: A higher proportion of fetuses with diaphragmatic eventration had associated pleural and pericardial effusions compared with fetuses with diaphragmatic hernia (58% (7/12) vs. 3.7% (14/382), respectively, P < 0.001). This observation remained true when only cases of diaphragmatic defects not associated with hydrops and other major structural or chromosomal anomalies were compared (29% (2/7) with eventration vs. 2.2% (4/178) with CDH, P < 0.02).
Conclusions: The presence of pleural and/or pericardial effusion in patients with diaphragmatic defects should raise the possibility of a congenital diaphragmatic eventration. This information is clinically important for management and counseling because the prognosis and treatment for CDH and congenital diaphragmatic eventration are different. Published by John Wiley & Sons, Ltd.
Copyright (c) 2007 ISUOG.
Figures
Similar articles
-
Left diaphragmatic eventration diagnosed as congenital diaphragmatic hernia by prenatal sonography.J Clin Ultrasound. 2003 May;31(4):214-7. doi: 10.1002/jcu.10157. J Clin Ultrasound. 2003. PMID: 12692831
-
An unusual hernia: congenital pericardial effusion associated with liver herniation into the pericardial sac.Pediatr Radiol. 1996 Nov;26(11):791-3. doi: 10.1007/BF01396203. Pediatr Radiol. 1996. PMID: 8929379
-
Fetal diaphragmatic hernia presented with transient unilateral pleural effusion.Ultrasound Obstet Gynecol. 1997 Feb;9(2):125-7. doi: 10.1046/j.1469-0705.1997.09020125.x. Ultrasound Obstet Gynecol. 1997. PMID: 9132255
-
A congenital anterior diaphragmatic hernia with massive pericardial effusion requiring neither emergency pericardiocentesis nor operation. A case report and review of the literature.J Perinat Med. 2002;30(4):336-40. doi: 10.1515/JPM.2002.050. J Perinat Med. 2002. PMID: 12235724 Review.
-
Diaphragmatic eventration presenting as a recurrent diaphragmatic hernia.Ann R Coll Surg Engl. 2017 Sep;99(7):e196-e199. doi: 10.1308/rcsann.2016.0342. Ann R Coll Surg Engl. 2017. PMID: 28853592 Free PMC article. Review.
Cited by
-
Current advances in prenatal imaging of congenital diaphragmatic [corrected] hernia.Pediatr Radiol. 2012 Jan;42 Suppl 1:S74-90. doi: 10.1007/s00247-011-2183-3. Epub 2011 Jul 8. Pediatr Radiol. 2012. PMID: 21739292
-
Prenatal diagnosis of bilateral pulmonary agenesis: a case report.Korean J Radiol. 2010 Jan-Feb;11(1):119-22. doi: 10.3348/kjr.2010.11.1.119. Epub 2009 Dec 28. Korean J Radiol. 2010. PMID: 20046503 Free PMC article.
References
-
- Adzick NS, Vacanti JP, Lillehei CW, O'Rourke PP, Crone RK, Wilson JM. Fetal diaphragmatic hernia: ultrasound diagnosis and clinical outcome in 38 cases. J Pediatr Surg. 1989;24:654–657. - PubMed
-
- Bagolan P, Casaccia G, Crescenzi F, Nahom A, Trucchi A, Giorlandino C. Impact of a current treatment protocol on outcome of high-risk congenital diaphragmatic hernia. J Pediatr Surg. 2004;39:313–318. - PubMed
-
- Bedoyan JK, Blackwell SC, Treadwell MC, Johnson A, Klein MD. Congenital diaphragmatic hernia: associated anomalies and antenatal diagnosis. Outcome-related variables at two Detroit hospitals. Pediatr Surg Int. 2004;20:170–176. - PubMed
-
- Colvin J, Bower C, Dickinson JE, Sokol J. Outcomes of congenital diaphragmatic hernia: a population-based study in Western Australia. Pediatrics. 2005;116:e356–e363. - PubMed
-
- Graham G, Devine PC. Antenatal diagnosis of congenital diaphragmatic hernia. Semin Perinatol. 2005;29:69–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
