

Volumetric assessment of tumor infiltration of adjacent white matter based on anatomic MRI and diffusion tensor tractography
- PMID: 17368212
- PMCID: PMC2397554
- DOI: 10.1016/j.acra.2007.01.033
Volumetric assessment of tumor infiltration of adjacent white matter based on anatomic MRI and diffusion tensor tractography
Abstract
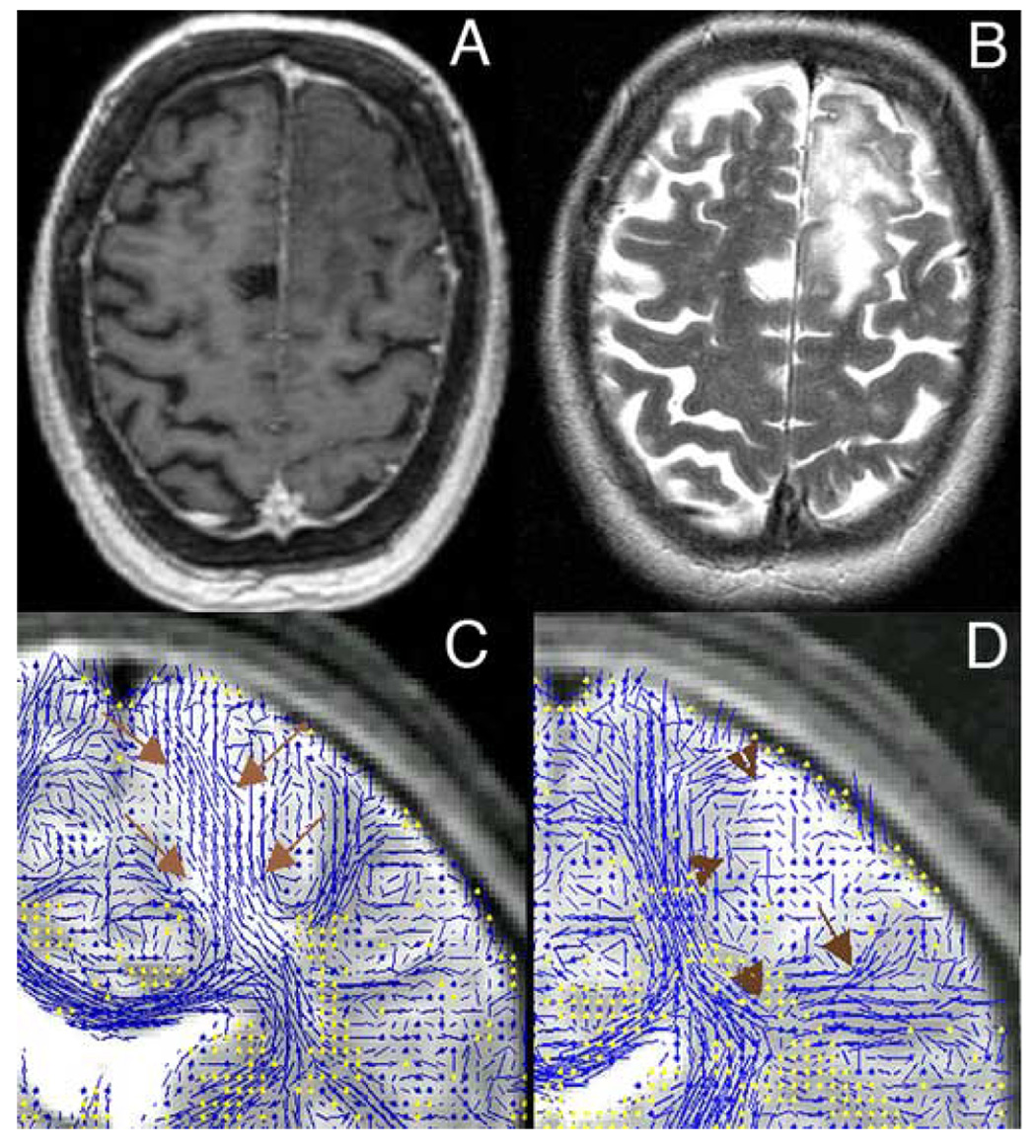
Rationale and objectives: To perform a retrospective, quantitative assessment of the anatomic relationship between intra-axial, supratentorial, primary brain tumors, and adjacent white matter fiber tracts based on anatomic and diffusion tensor magnetic resonance imaging (MRI). We hypothesized that white matter infiltration may be common among different types of tumor.
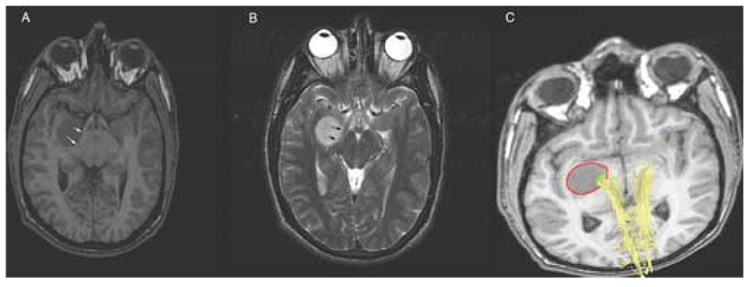
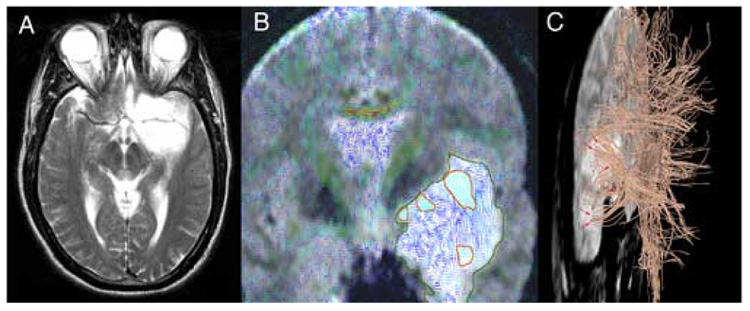
Material and methods: Preoperative, anatomic (T1- and T2-weighted), and LINESCAN diffusion tensor MRI were obtained in 12 patients harboring supratentorial gliomas (World Health Organization [WHO] Grades II and III). The two imaging modalities were rigidly registered. The tumors were manually segmented from the T1- and T2-weighted MRI, and their volume calculated. A three-dimensional tractography was performed in each case. A second segmentation and volume measurement was performed on the tumor regions intersecting adjacent white matter fiber tracts. Statistical methods included summary statistics to examine the fraction of tumor volume infiltrating adjacent white matter.
Results: There were five patients with low-grade oligodendroglioma (WHO Grade II), one with low-grade mixed oligoastrocytoma (WHO Grade II), one with ganglioglioma, two with low-grade astrocytoma (WHO Grade II), and three with anaplastic astrocytoma (WHO Grade III). We identified white matter tracts infiltrated by tumor in all 12 cases. The median tumor volume (+/- standard deviation) in our patient population was 42.5 +/- 28.9 mL. The median tumor volume (+/- standard deviation) infiltrating white matter fiber tracts was 5.2 +/- 9.9 mL. The median percentage of tumor volume infiltrating white matter fiber tracts was 21.4% +/- 9.7%.
Conclusions: The information provided by diffusion tensor imaging combined with anatomic MRI might be useful for neurosurgical planning and intraoperative guidance. Our results confirm previous reports that extensive white matter infiltration by primary brain tumors is a common occurrence. However, prospective, large population studies are required to definitively clarify this issue, and how infiltration relates to histologic tumor type, tumor size, and location.
Figures
Similar articles
-
Generalized q-sampling imaging fiber tractography reveals displacement and infiltration of fiber tracts in low-grade gliomas.Neuroradiology. 2018 Mar;60(3):267-280. doi: 10.1007/s00234-018-1985-5. Epub 2018 Jan 25. Neuroradiology. 2018. PMID: 29372286
-
[Application of diffusion tensor imaging in preoperation and postoperation patients of glioma with 3.0 Tesla MRI].Zhonghua Yi Xue Za Zhi. 2009 May 19;89(19):1300-4. Zhonghua Yi Xue Za Zhi. 2009. PMID: 19615179 Chinese.
-
Revisiting anaplastic astrocytomas II: further characterization of an expansive growth pattern with visually enhanced diffusion tensor imaging.J Magn Reson Imaging. 2008 Dec;28(6):1322-36. doi: 10.1002/jmri.21594. J Magn Reson Imaging. 2008. PMID: 19025901
-
High-definition fiber tractography for the evaluation of perilesional white matter tracts in high-grade glioma surgery.Neuro Oncol. 2015 Sep;17(9):1199-209. doi: 10.1093/neuonc/nov113. Epub 2015 Jun 27. Neuro Oncol. 2015. PMID: 26117712 Free PMC article. Review.
-
High-Definition Fiber Tractography in Evaluation and Surgical Planning of Thalamopeduncular Pilocytic Astrocytomas in Pediatric Population: Case Series and Review of Literature.World Neurosurg. 2017 Feb;98:463-469. doi: 10.1016/j.wneu.2016.11.061. Epub 2016 Nov 22. World Neurosurg. 2017. PMID: 27888085 Review.
Cited by
-
Generalized q-sampling imaging fiber tractography reveals displacement and infiltration of fiber tracts in low-grade gliomas.Neuroradiology. 2018 Mar;60(3):267-280. doi: 10.1007/s00234-018-1985-5. Epub 2018 Jan 25. Neuroradiology. 2018. PMID: 29372286
-
Surgical impact on brain tumor invasion: a physical perspective.Ann Surg Innov Res. 2008 Apr 2;2:1. doi: 10.1186/1750-1164-2-1. Ann Surg Innov Res. 2008. PMID: 18384681 Free PMC article.
-
Imaging of central nervous system tumors in children: advances and limitations.J Child Neurol. 2008 Oct;23(10):1128-35. doi: 10.1177/0883073808320753. J Child Neurol. 2008. PMID: 18952579 Free PMC article. Review.
-
The Disruption of Geniculocalcarine Tract in Occipital Neoplasm: A Diffusion Tensor Imaging Study.Radiol Res Pract. 2016;2016:8213076. doi: 10.1155/2016/8213076. Epub 2016 Aug 16. Radiol Res Pract. 2016. PMID: 27610244 Free PMC article.
-
Tractography for Surgical Neuro-Oncology Planning: Towards a Gold Standard.Neurotherapeutics. 2019 Jan;16(1):36-51. doi: 10.1007/s13311-018-00697-x. Neurotherapeutics. 2019. PMID: 30542904 Free PMC article. Review.
References
-
- Central Brain Tumor Registry of The United States. Statistical Report: Primary Brain Tumors in The United States 1998–2002. Primary Brain Tumors in The United States 1998–2002. 2005. http://cbtrus.org/reports//2005–2006/2006report.pdf.
-
- Nicolato A, Gerosa MA, Fina P, Iuzzolino P, et al. Prognostic factors in low-grade supratentorial astrocytomas: a uni-multivariate statistical analysis in 76 surgically treated adult patients. Surg Neurol. 1995;44(3):208–221. discussion 221-3. - PubMed
-
- Pignatti F, van den Bent M, Curran D, Debruyne C, et al. Prognostic factors for survival in adult patients with cerebral low-grade glioma. J Clin Oncol. 2002;20(8):2076–2084. - PubMed
-
- Janny P, Cure H, Mohr M, Heldt N, et al. Low grade supratentorial astrocytomas. Management and prognostic factors. Cancer. 1994;73(7):1937–1945. - PubMed
-
- Keles GE, Lamborn KR, Berger MS. Low-grade hemispheric gliomas in adults: a critical review of extent of resection as a factor influencing outcome. J Neurosurg. 2001;95(5):735–745. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
