

Statin use and breast cancer risk in a large population-based setting
- PMID: 17372235
- PMCID: PMC2065858
- DOI: 10.1158/1055-9965.EPI-06-0737
Statin use and breast cancer risk in a large population-based setting
Abstract
Background: Mechanistic studies suggest that 3-hydroxy-3-methylglutaryl CoA inhibitors (statins) reduce the risk of breast cancer. Observational studies offer mixed results.
Methods: To evaluate the relation between statin use and breast cancer risk, we conducted a cohort study among women ages 45 to 89 years within an integrated health care delivery system. Information on statin use and covariates were obtained from automated databases. We identified breast cancer cases through the Surveillance, Epidemiology, and End Results registry. We used Cox proportional hazards models to estimate the hazard ratios (HR) and 95% confidence intervals (95% CI) for invasive breast cancer among statin users compared with nonusers.
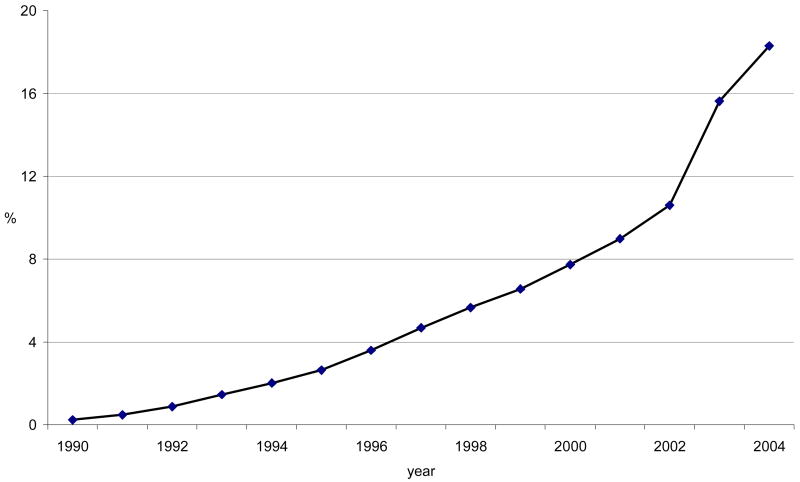
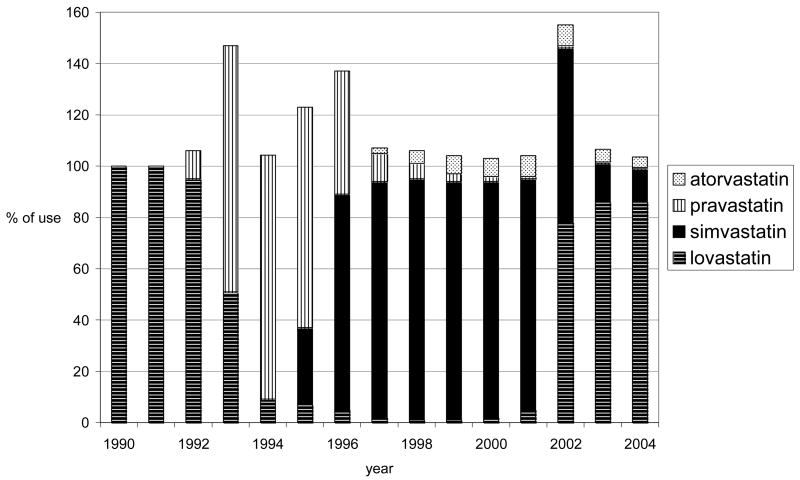
Results: Among 92,788 women studied from 1990 to 2004, median follow-up time was 6.4 years, and 2,707 breast cancer cases were identified. During the study period, 7.4% of women used statins for at least 1 year, and the median duration of use was 3.1 years. We found no difference in breast cancer risk among statin users (HR, 1.07; 95% CI, 0.88-1.29) compared with nonusers. Risk of breast cancer did not differ by duration of use (1-2.9, 3-4.9, or >or=5 years) or hydrophobic statin use. We found a suggestive increased risk of breast cancer among statin users of >or=5 years (HR, 1.27; 95% CI, 0.89-1.81 for any statins and HR, 1.47; 95% CI, 0.89-2.44 for hydrophobic statins) and of estrogen receptor-negative tumors with increasing duration of statin use (1-2.9 years: HR, 1.33; 95% CI, 0.64-2.77; 3-4.9 years: HR, 1.68; 95% CI, 0.72-3.92; >or=5 years: HR, 1.81; 95% CI, 0.75-4.36).
Conclusion: This study does not support an association between statin use and breast cancer risk.
Figures
References
-
- Sewester CS, Dombek CE, Olin BR, Kastrup EK, Hebel SK. Drug Facts and Comparisons. St. Louis, MO; 2004.
-
- RX List. The Top 200 Prescriptions for 2004 by U.S. Sales. [Accessed May 10, 2005]. Available at: http://www.rxlist.com/top200_sales_2004.
-
- Newman TB, Hulley SB. Carcinogenicity of lipid-lowering drugs. JAMA. 1996;275:55–60. - PubMed
-
- Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med. 1996;335:1001–9. - PubMed
-
- Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360:1623–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
