

Avoidable mortality by neighbourhood income in Canada: 25 years after the establishment of universal health insurance
- PMID: 17372287
- PMCID: PMC2652935
- DOI: 10.1136/jech.2006.047092
Avoidable mortality by neighbourhood income in Canada: 25 years after the establishment of universal health insurance
Abstract
Aim: To examine neighbourhood income differences in deaths amenable to medical care and public health over a 25-year period after the establishment of universal insurance for doctors and hospital services in Canada.
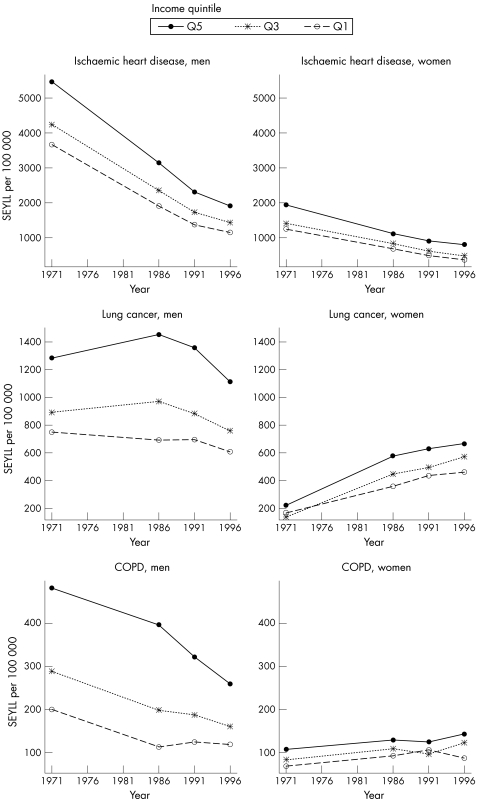
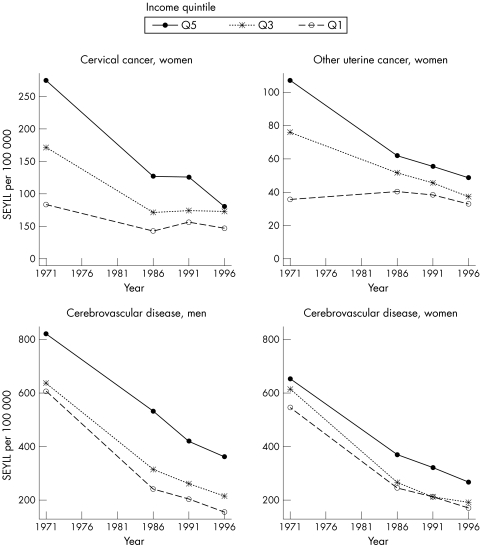
Methods: Data for census metropolitan areas were obtained from the Canadian Mortality Database and population censuses for the years 1971, 1986, 1991 and 1996. Deaths amenable to medical care, amenable to public health, from ischaemic heart disease and from other causes were considered. Data on deaths were grouped into neighbourhood income quintiles on the basis of the census tract percentage of population below Canada's low-income cut-offs.
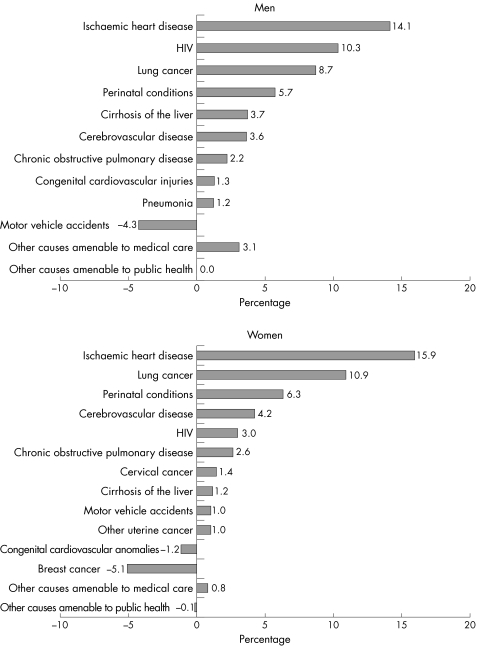
Results: From 1971 to 1996, differences between the richest and poorest quintiles in age-standardised expected years of life lost amenable to medical care decreased 60% (p<0.001) in men and 78% (p<0.001) in women, those amenable to public health increased 0.7% (p = 0.94) in men and 20% (p = 0.55) in women, those lost from ischaemic heart disease decreased 58% in men and 38% in women, and from other causes decreased 15% in men and 9% in women. Changes in the age-standardised expected years of life lost difference for deaths amenable to medical care were significantly larger than those for deaths amenable to public health or other causes for both men and women (p<0.001).
Conclusions: Reductions in rates of deaths amenable to medical care made the largest contribution to narrowing socioeconomic mortality disparities. Continuing disparities in mortality from causes amenable to public health suggest that public health initiatives have a potentially important, but yet un-realized, role in further reducing mortality disparities in Canada.
Conflict of interest statement
Competing interests: None declared.


Similar articles
-
Changes in mortality by income in urban Canada from 1971 to 1986.Health Rep. 1989;1(2):137-74. Health Rep. 1989. PMID: 2491131 English, French.
-
The East-West life expectancy gap: differences in mortality from conditions amenable to medical intervention.Int J Epidemiol. 1997 Feb;26(1):75-84. doi: 10.1093/ije/26.1.75. Int J Epidemiol. 1997. PMID: 9126506
-
The contribution of health policy and care to income differences in life expectancy--a register based cohort study.BMC Public Health. 2013 Sep 8;13:812. doi: 10.1186/1471-2458-13-812. BMC Public Health. 2013. PMID: 24010957 Free PMC article.
-
Mortality due to low-quality health systems in the universal health coverage era: a systematic analysis of amenable deaths in 137 countries.Lancet. 2018 Nov 17;392(10160):2203-2212. doi: 10.1016/S0140-6736(18)31668-4. Epub 2018 Sep 5. Lancet. 2018. PMID: 30195398 Free PMC article.
-
Amenable Mortality in Children under 5: An Indicator for Identifying Inequalities in Healthcare Delivery: A Review.Children (Basel). 2024 Jun 24;11(7):764. doi: 10.3390/children11070764. Children (Basel). 2024. PMID: 39062214 Free PMC article. Review.
Cited by
-
A Structural Equation Model of HIV-Related Stigma, Racial Discrimination, Housing Insecurity and Wellbeing among African and Caribbean Black Women Living with HIV in Ontario, Canada.PLoS One. 2016 Sep 26;11(9):e0162826. doi: 10.1371/journal.pone.0162826. eCollection 2016. PLoS One. 2016. PMID: 27669510 Free PMC article.
-
Neighborhood context and infant birthweight among recent immigrant mothers: a multilevel analysis.Am J Public Health. 2009 Feb;99(2):285-93. doi: 10.2105/AJPH.2007.127498. Epub 2008 Dec 4. Am J Public Health. 2009. PMID: 19059866 Free PMC article.
-
Primary payer status is associated with mortality and resource utilization for coronary artery bypass grafting.Circulation. 2012 Sep 11;126(11 Suppl 1):S132-9. doi: 10.1161/CIRCULATIONAHA.111.083782. Circulation. 2012. PMID: 22965973 Free PMC article.
-
How much do local health systems matter? Variations in amenable mortality across health districts in Aotearoa New Zealand.Public Health Pract (Oxf). 2024 Aug 26;8:100545. doi: 10.1016/j.puhip.2024.100545. eCollection 2024 Dec. Public Health Pract (Oxf). 2024. PMID: 39309249 Free PMC article. No abstract available.
-
Pharmacy location and medical need: regional evidence from Canada.BMC Health Serv Res. 2022 Nov 3;22(1):1309. doi: 10.1186/s12913-022-08709-5. BMC Health Serv Res. 2022. PMID: 36329439 Free PMC article.
References
-
- Canada Health Act, ch C–6, §10. 1984
-
- Detsky A S, Naylor C D. Canada's health care system—reform delayed. N Engl J Med 2003349804–810. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources