

Chronic pain in Canada: have we improved our management of chronic noncancer pain?
- PMID: 17372633
- PMCID: PMC2670724
- DOI: 10.1155/2007/762180
Chronic pain in Canada: have we improved our management of chronic noncancer pain?
Abstract
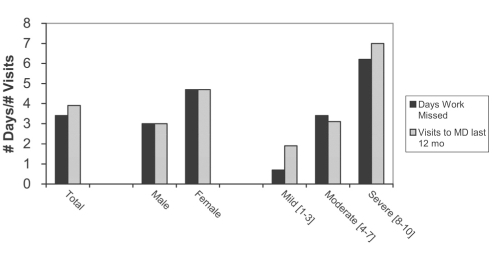
Background: Chronic noncancer pain (CNCP) is a global issue, not only affecting individual suffering, but also impacting the delivery of health care and the strength of local economies.
Objectives: The current study (the Canadian Chronic Pain Study II [CCPSII]) was designed to assess any changes in the prevalence and treatment of CNCP, as well as in attitudes toward the use of strong analgesics, compared with a 2001 study (the CCPSI), and to provide a snapshot of the current standards of care for pain management in Canada.
Methods: Standard, computer-assisted telephone interview survey methodology was applied in two segments, ie, a general population survey and a survey targeting randomly selected primary care physicians (PCPs) who treat moderate to severe CNCP.
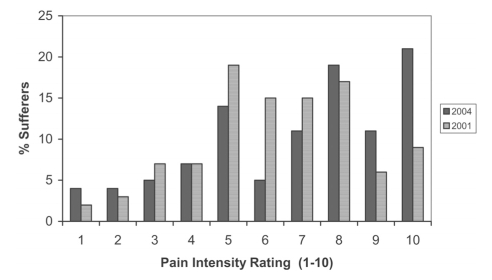
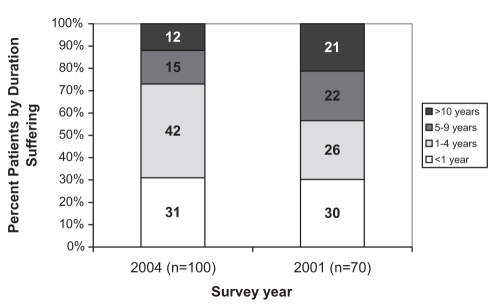
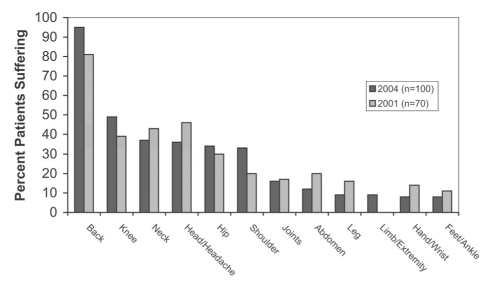
Results and discussion: The patient-reported prevalence of CNCP within Canada has not markedly changed since 2001 but the duration of suffering has decreased. There have been minor changes in regional distribution and generally more patients receive medical treatment, which includes prescription analgesics. Physicians continue to demonstrate opiophobia in their prescribing practices; however, although this is lessened relating to addiction, abuse remains an important concern to PCPs. Canadian PCPs, in general, are implementing standard assessments, treatment approaches, evaluation of treatment success and tools to prevent abuse and diversion, in accordance with guidelines from the Canadian Pain Society and other pain societies globally, although there remains room for improvement and standardization.
HISTORIQUE :: La douleur chronique non cancéreuse (DCNC) est un problème global qui n’affecte pas seulement la personne souffrante, mais également la prestation des soins de santé et la vigueur des économies locales.
OBJECTIFS :: La présente étude (CCPS II [Canadian Chronic Pain Study II]) a été conçue pour mesurer, le cas échéant, les changements qui ont influé sur la prévalence et le traitement de la DCNC, de même que sur les attitudes vis-à-vis du recours aux analgésiques puissants, comparativement à une étude réalisée en 2001 (l’étude CCPS I) et dresser un portrait des normes actuelles en matière de contrôle de la douleur au Canada.
MÉTHODE :: Méthodologie d’enquête standard par entrevue téléphonique assistée par ordinateur, appliquée à deux segments de population, soit enquête auprès de la population générale et enquête auprès d’omnipraticiens qui soignent la DCNC de modérée à sévère sélectionnés au hasard.
RÉSULTATS ET DISCUSSION :: La prévalence de la DCNC telle qu’elle est signalée par les patients au Canada n’a pas sensiblement changé depuis 2001, mais la durée de la douleur a diminué. On a noté des changements mineurs quant à la distribution régionale et en général, un plus grand nombre de patients reçoivent un traitement médical qui inclut des analgésiques vendus sur ordonnance. Les habitudes de prescription des médecins continuent de témoigner de leur « opiophobie ». Par contre, bien que celle-ci semble moins associée à la peur de la dépendance, les risques d’abus continuent de préoccuper les omnipraticiens. Les omnipraticiens canadiens appliquent généralement les techniques d’examen, les approches thérapeutiques, les évaluations de traitement et les outils standard pour prévenir les abus et autres usages illicites, conformément aux directives de la Société canadienne pour le traitement de la douleur et d’autres sociétés apparentées à l’échelle globale. Mais il y a toujours place pour l’amélioration et la standardisation.
Figures
References
-
- Moulin DE, Clark AJ, Speechley M, Morley-Forster MK. Chronic Pain in Canada – prevalence, treatment, impact and the role of opioid analgesia. Pain Res Manage. 2002;7:179–84. - PubMed
-
- Van Den Kerkhof EG, Hopman WM, Towheed TE, Anastassiades TP, Goldstein DH, Canadian Multicentre Osteoporosis Study Research Group The impact of sampling and measurement on the prevalence of self-reported pain in Canada. Pain Res Manage. 2003;8:157–63. - PubMed
-
- Stannard C, Johnson M. Chronic pain management – can we do better? An interview-based survey in primary care. Curr Med Res Opin. 2003;19:703–6. - PubMed
-
- Marcus DA. Managing chronic pain in the primary care setting. Amer Fam Physician. 2002;66:36–41. - PubMed
-
- Blyth FM, March LM, Brnabic AJ, Cousins MJ. Chronic pain and frequent use of health care. Pain. 2004;111:51–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
