

Changes in preferences for life-sustaining treatment among older persons with advanced illness
- PMID: 17372799
- PMCID: PMC1839865
- DOI: 10.1007/s11606-007-0104-9
Changes in preferences for life-sustaining treatment among older persons with advanced illness
Abstract
Background: There are conflicting assumptions regarding how patients' preferences for life-sustaining treatment change over the course of serious illness.
Objective: To examine changes in treatment preferences over time.
Design: Longitudinal cohort study with 2-year follow-up.
Participants: Two hundred twenty-six community-dwelling persons age > or =60 years with advanced cancer, congestive heart failure, or chronic obstructive pulmonary disease.
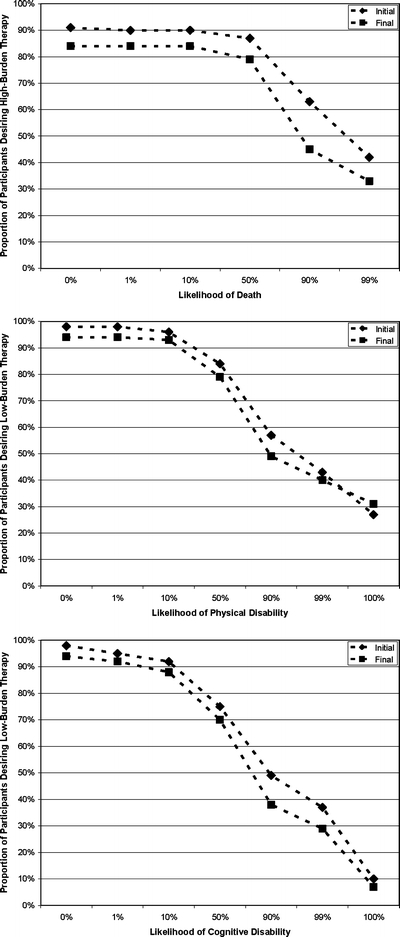
Measurements: Participants were asked, if faced with an illness exacerbation that would be fatal if untreated, whether they would: a) undergo high-burden treatment at a given likelihood of death and b) undergo low-burden treatment at a given likelihood of severe disability, versus a return to current health.
Results: There was little change in the overall proportions of participants who would undergo therapy at a given likelihood of death or disability from first to final interview. Diversity within the population regarding the highest likelihood of death or disability at which the individual would undergo therapy remained substantial over time. Despite a small magnitude of change, the odds of participants' willingness to undergo high-burden therapy at a given likelihood of death and to undergo low-burden therapy at a given likelihood of severe cognitive disability decreased significantly over time. Greater functional disability, poorer quality of life, and lower self-rated life expectancy were associated with decreased willingness to undergo therapy.
Conclusions: Diversity among older persons with advanced illness regarding treatment preferences persists over time. Although the magnitude of change is small, there is a decreased willingness to undergo highly burdensome therapy or to risk severe disability in order to avoid death over time and with declining health status.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1056/NEJM199607183350306', 'is_inner': False, 'url': 'https://doi.org/10.1056/nejm199607183350306'}, {'type': 'PubMed', 'value': '8657216', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8657216/'}]}
- Christakis NA, Escarce JJ. Survival of Medicare patients after enrollment in hospice programs. N Engl J Med. 1996;335:172–8. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1056/NEJM200204043461413', 'is_inner': False, 'url': 'https://doi.org/10.1056/nejm200204043461413'}, {'type': 'PubMed', 'value': '11932479', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11932479/'}]}
- Meier DE, Morrison RS. Autonomy reconsidered. N Engl J Med. 2002;346:1087–9. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1001/jama.282.17.1670', 'is_inner': False, 'url': 'https://doi.org/10.1001/jama.282.17.1670'}, {'type': 'PubMed', 'value': '10553796', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10553796/'}]}
- Finucane TE. How gravely ill becomes dying: a key to end-of-life care. JAMA. 1999;282:1670–2. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '8116994', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8116994/'}]}
- Danis M, Garrett J, Harris R, Patrick DL. Stability of choices about life-sustaining treatments. Ann Intern Med. 1994;120:567–73. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1111/j.1532-5415.2004.52165.x', 'is_inner': False, 'url': 'https://doi.org/10.1111/j.1532-5415.2004.52165.x'}, {'type': 'PubMed', 'value': '15066074', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15066074/'}]}
- Straton JB, Wang NY, Meoni LA, et al. Physical functioning, depression, and preferences for treatment at the end of life: the Johns Hopkins Precursors Study. J Am Geriatr Soc. 2004;52:577–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
