

Flow mediated dilation of the brachial artery: an investigation of methods requiring further standardization
- PMID: 17376239
- PMCID: PMC1847451
- DOI: 10.1186/1471-2261-7-11
Flow mediated dilation of the brachial artery: an investigation of methods requiring further standardization
Abstract
Background: In order to establish a consistent method for brachial artery reactivity assessment, we analyzed commonly used approaches to the test and their effects on the magnitude and time-course of flow mediated dilation (FMD), and on test variability and repeatability. As a popular and noninvasive assessment of endothelial function, several different approaches have been employed to measure brachial artery reactivity with B-mode ultrasound. Despite some efforts, there remains a lack of defined normal values and large variability in measurement technique.
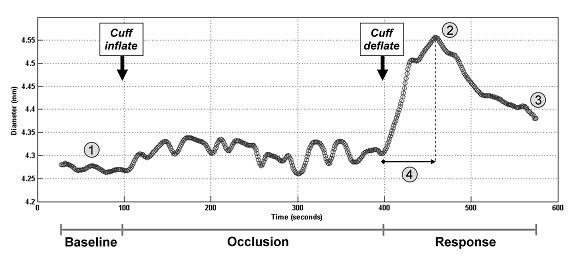
Methods: Twenty-six healthy volunteers underwent repeated brachial artery diameter measurements by B-mode ultrasound. Following baseline diameter recordings we assessed endothelium-dependent flow mediated dilation by inflating a blood pressure cuff either on the upper arm (proximal) or on the forearm (distal).
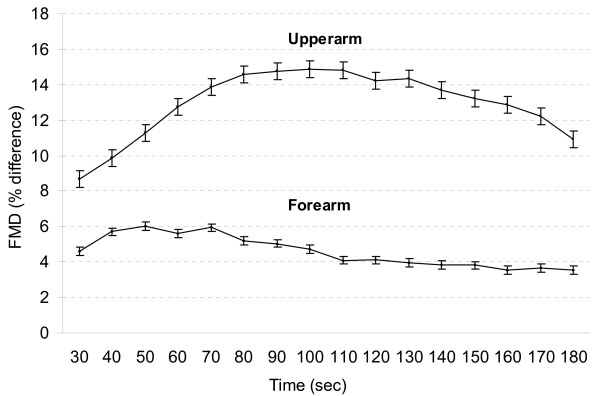
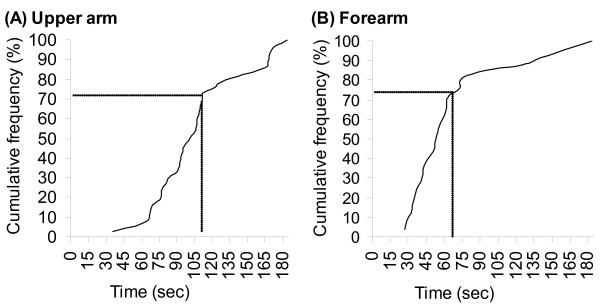
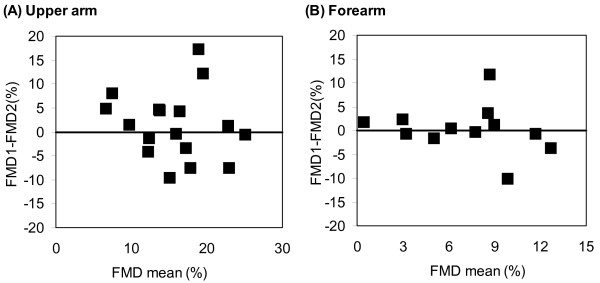
Results: Thirty-seven measures were performed using proximal occlusion and 25 with distal occlusion. Following proximal occlusion relative to distal occlusion, FMD was larger (16.2 +/- 1.2% vs. 7.3 +/- 0.9%, p < 0.0001) and elongated (107.2 s vs. 67.8 s, p = 0.0001). Measurement of the test repeatability showed that differences between the repeated measures were greater on average when the measurements were done using the proximal method as compared to the distal method (2.4%; 95% CI 0.5-4.3; p = 0.013).
Conclusion: These findings suggest that forearm compression holds statistical advantages over upper arm compression. Added to documented physiological and practical reasons, we propose that future studies should use forearm compression in the assessment of endothelial function.
Figures
Similar articles
-
Noninvasive assessment of endothelium-dependent flow-mediated dilation of the brachial artery.Vasc Med. 1997;2(2):87-92. doi: 10.1177/1358863X9700200203. Vasc Med. 1997. PMID: 9546961
-
Comparison of ultrasound assessment of flow-mediated dilatation in the radial and brachial artery with upper and forearm cuff positions.Clin Physiol. 2001 Jan;21(1):9-14. doi: 10.1046/j.1365-2281.2001.00302.x. Clin Physiol. 2001. PMID: 11168291
-
Occlusion cuff position is an important determinant of the time course and magnitude of human brachial artery flow-mediated dilation.Clin Sci (Lond). 2000 Oct;99(4):261-7. Clin Sci (Lond). 2000. PMID: 10995590 Clinical Trial.
-
Assessment of flow-mediated vasodilatation (FMD) of the brachial artery: effects of technical aspects of the FMD measurement on the FMD response.Eur Heart J. 2005 Feb;26(4):363-8. doi: 10.1093/eurheartj/ehi017. Epub 2004 Dec 1. Eur Heart J. 2005. PMID: 15618057 Review.
-
Detection of endothelial dysfunction with brachial artery ultrasound scanning.Am Heart J. 2003 Jun;145(6):943-51. doi: 10.1016/S0002-8703(03)00097-8. Am Heart J. 2003. PMID: 12796748 Review.
Cited by
-
The effect of low and high-intensity cycling in diesel exhaust on flow-mediated dilation, circulating NOx, endothelin-1 and blood pressure.PLoS One. 2018 Feb 21;13(2):e0192419. doi: 10.1371/journal.pone.0192419. eCollection 2018. PLoS One. 2018. PMID: 29466393 Free PMC article.
-
Assessment of flow-mediated dilation in humans: a methodological and physiological guideline.Am J Physiol Heart Circ Physiol. 2011 Jan;300(1):H2-12. doi: 10.1152/ajpheart.00471.2010. Epub 2010 Oct 15. Am J Physiol Heart Circ Physiol. 2011. PMID: 20952670 Free PMC article. Review.
-
Brachial artery flow-mediated dilation in patients with systemic sclerosis: an experience from tertiary care center from North India.Clin Rheumatol. 2023 Jul;42(7):1827-1832. doi: 10.1007/s10067-023-06562-3. Epub 2023 Mar 10. Clin Rheumatol. 2023. PMID: 36897457
-
A Pilot Study to Determine if Vitamin D Repletion Improves Endothelial Function in Lupus Patients.Am J Med Sci. 2015 Oct;350(4):302-7. doi: 10.1097/MAJ.0000000000000556. Am J Med Sci. 2015. PMID: 26351776 Free PMC article. Clinical Trial.
-
Myeloperoxidase impacts vascular function by altering perivascular adipocytes' secretome and phenotype in obesity.Cell Rep Med. 2025 May 20;6(5):102087. doi: 10.1016/j.xcrm.2025.102087. Epub 2025 Apr 18. Cell Rep Med. 2025. PMID: 40252642 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
