

Review
doi: 10.1016/j.bbamem.2007.02.010.
Epub 2007 Feb 20.
Cardiac GPCRs: GPCR signaling in healthy and failing hearts
Affiliations
- PMID: 17376402
- PMCID: PMC1892229
- DOI: 10.1016/j.bbamem.2007.02.010
Item in Clipboard
Review
Cardiac GPCRs: GPCR signaling in healthy and failing hearts
Biochim Biophys Acta.
2007 Apr.
Abstract
G protein-coupled receptors (GPCRs) are widely implicated in human heart disease, making them an important target for cardiac drug therapy. The most commonly studied and clinically targeted cardiac GPCRs include the adrenergic, angiotensin, endothelin, and adenosine receptors. Treatment options focusing on the complex and integrated signaling pathways of these GPCRs are critical for the understanding and amelioration of heart disease. The focus of this review is to highlight the most commonly studied and clinically targeted cardiac GPCRs, placing emphasis on their common signaling components implicated in cardiac disease.
Figures
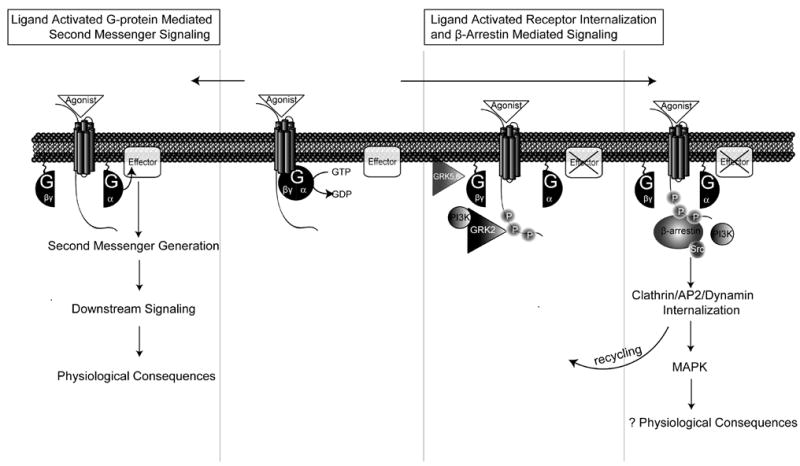
Agonist binding to receptor results in the coupling to a G-protein and the conversion of GTP to GDP to cause the dissociation of Gα and Gβγ subunits. Gα signaling is initiated with the activation of a membrane-bound effector molecule, such as adenylyl cyclase (AC) or phospholipase C β (PLCβ) to produce second messengers such as cyclic adenosine 3′,5′ monophosphate, (cAMP), diacylglycerol (DAG), or inositol 1,4, 5-triphosphate (IP3), which activate a variety of downstream signals with a range of physiological consequences in the heart such as the regulation of contractility, hypertrophy, and apoptosis. A simultaneous process involves the ligand-activated translocation of G protein-coupled receptor kinases (GRKs) and bound phosphoinositide-3-kinase (PI3K), to the membrane by dissociated Gβγ subunits leading to receptor phosphorylation on the C-terminal tail. Following GRK mediated receptor phosphorylation, β-arrestin is bound and acts to 1) desensitize G protein signaling by uncoupling the receptor from G protein, 2) scaffold for the recruitment of proteins involving in receptor trafficking, such as AP2, clathrin, and dynamin, and 3) form a signaling complex that initiates G protein-independent downstream signaling such as the activation of mitogen-activated protein (MAP) kinases.
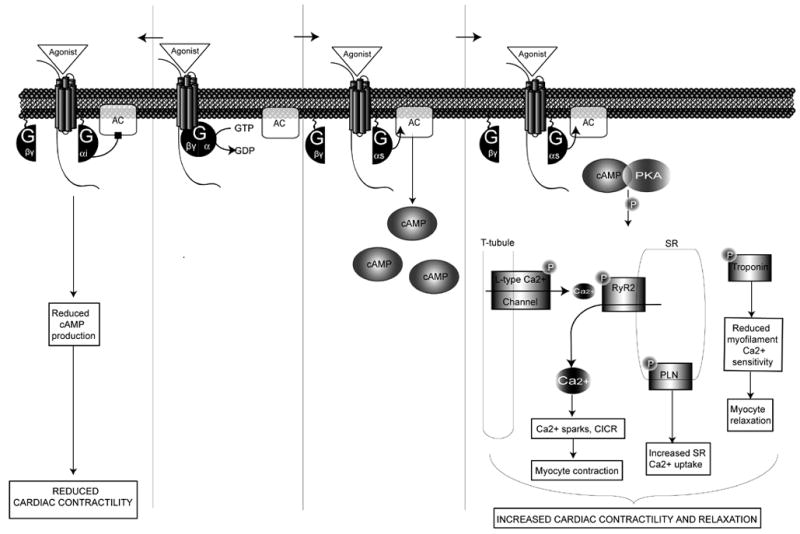
Gs- and Gi-coupled receptors target the second messenger adenylyl cyclase (AC). While Gs stimulates AC, activation of Gi inhibits AC, reducing the accumulation of cAMP and consequently leading to reduced PKA and agonist-stimulated cardiac contractility. Downstream effectors of Gαs activation result from the increase in PKA which phosphorylation substrates include: phospholamban (PLN), troponin, L-type Ca2+ channels, and the cardiac ryanodine receptor (RyR2).
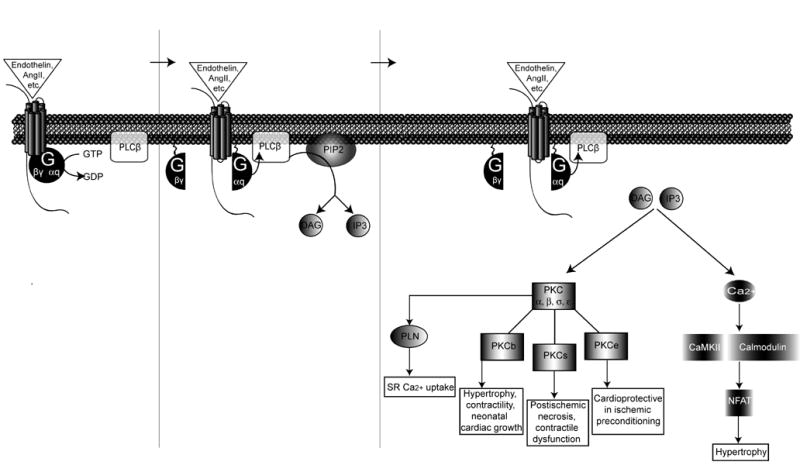
Gq-coupled receptors such as endothelin, angiotensin, or α-1-adrenergic receptors activate the second messenger phospholipase C β resulting in the hydrolysis of phosphatidylinositol 4, 5 biphosphate (PIP2) into two components: diacylglycerol (DAG) and inositol 1, 4, 5-triphosphate (IP3). DAG activates several isoforms of protein kinase C (PKC). PKCβ activation regulates hypertrophy, contractility, and neonatal cardiac growth. PKCσ activation regulates postischemic necrosis and contractile function. PKCε activation induces a cardioprotective effect in response to ischemic preconditioning. Activation of Gq-coupled receptors stimulates the release of calcium, which activates CaMKII and calcineurin to promote the nuclear translocation of nuclear factor of activated T-cells (NFAT) whereby the hypertrophic transcriptional machinery is activated.
References
-
- Pierce KL, Premont RT, Lefkowitz RJ. Nat Rev Mol Cell Biol. 2002;3:639–50. - PubMed
-
- Hopkins AL, Groom CR. Nat Rev Drug Discov. 2002;1:727–30. - PubMed
-
- Tang CM, Insel PA. Trends Cardiovasc Med. 2004;14:94–9. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW, Antman EM, Smith SC, Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. Circulation. 2005;112:e154–235. - PubMed
-
- Gether U, Kobilka BK. J Biol Chem. 1998;273:17979–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
