

The influence of volume and intensive care unit organization on hospital mortality in patients admitted with severe sepsis: a retrospective multicentre cohort study
- PMID: 17378934
- PMCID: PMC2206460
- DOI: 10.1186/cc5727
The influence of volume and intensive care unit organization on hospital mortality in patients admitted with severe sepsis: a retrospective multicentre cohort study
Abstract
Introduction: The aim of the study was to assess the influence of annual volume and factors related to intensive care unit (ICU) organization on in-hospital mortality among patients admitted to the ICU with severe sepsis.
Methods: A retrospective cohort study was conducted using the database of the Dutch National Intensive Care Evaluation (NICE) registry. Analyses were based on consecutive patients admitted between 1 January 2003 and 30 June 2005 who fulfilled criteria for severe sepsis within the first 24 hours of admission. A 13-item questionnaire was sent to all 32 ICUs across The Netherlands that participated in the NICE registry within this period in order to obtain information on ICU organization and staffing. The association between in-hospital mortality and factors related to ICU organization was investigated using logistic regression analysis, combined with generalized estimation equations to account for potential correlations of outcomes within ICUs. Correction for patient-related factors took place by including Simplified Acute Physiology Score II, age, sex and number of dysfunctioning organ systems in the analyses.
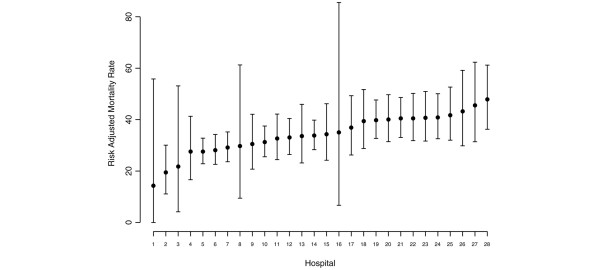
Results: Analyses based on 4,605 patients from 28 ICUs (questionnaire response rate 90.6%) revealed that a higher annual volume of severe sepsis patients is associated with a lower in-hospital mortality (P = 0.029). The presence of a medium care unit (MCU) as a step-down facility with intermediate care is associated with a higher in-hospital mortality (P = 0.013). For other items regarding ICU organization, no independent significant relationships with in-hospital mortality were found.
Conclusion: A larger annual volume of patients with severe sepsis admitted to Dutch ICUs is associated with lower in-hospital mortality in this patient group. The presence of a MCU as a step-down facility is associated with greater in-hospital mortality. No other significant associations between in-hospital mortality and factors related to ICU organization were found.
Figures
Comment in
-
Volume, outcome, and the organization of intensive care.Crit Care. 2007;11(3):129. doi: 10.1186/cc5776. Crit Care. 2007. PMID: 17493293 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
